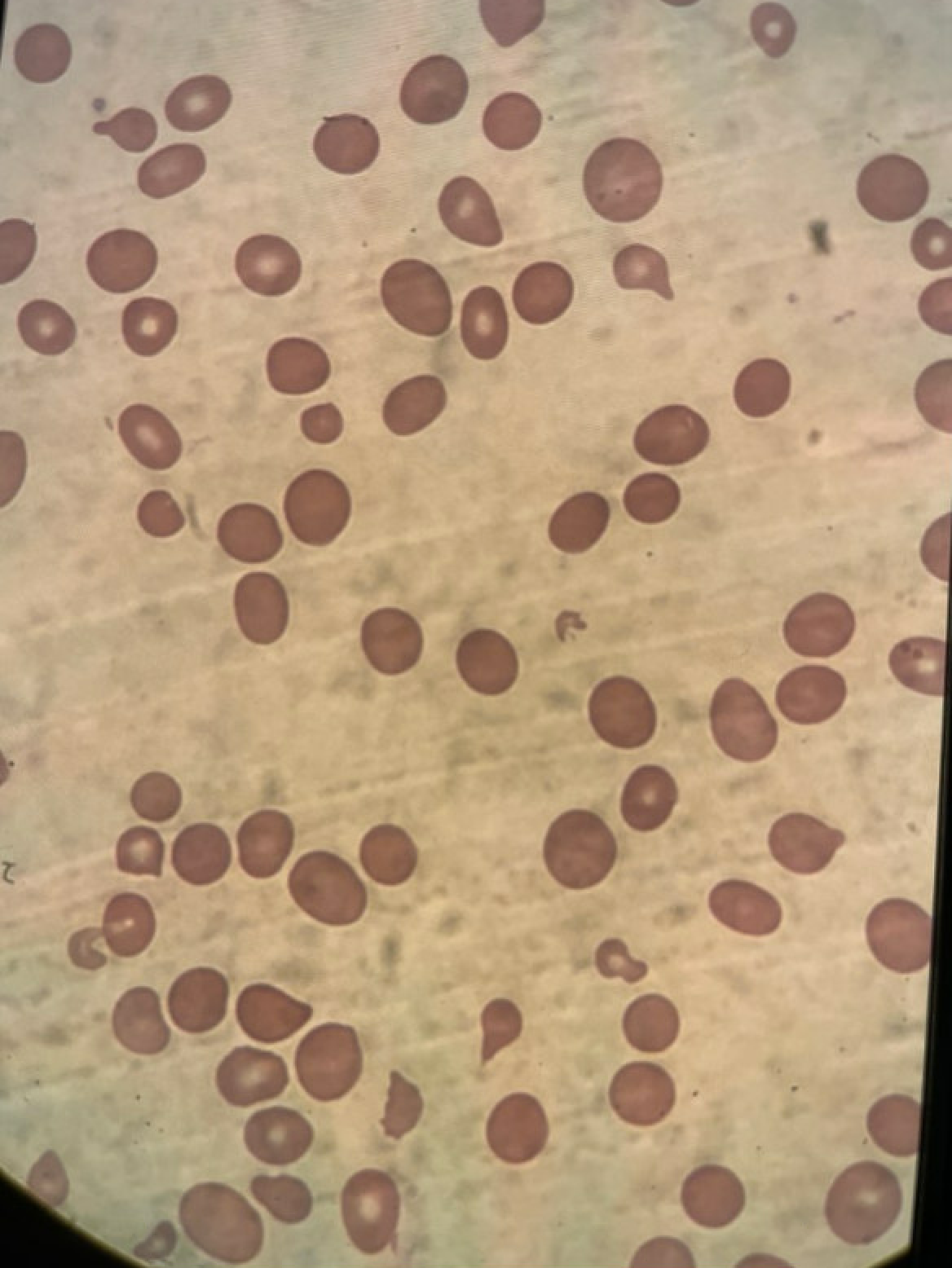
Case Presentation: A 40-year-old woman with a lifelong vegetarian diet presented to the emergency department (ED) with six weeks of progressive fatigue, exertional dyspnea, and anorexia. On arrival, she was tachycardic to 115 beats/minute but normotensive and well-appearing. Laboratory studies revealed severe macrocytic anemia (Hgb 5.5 g/dL, MCV 121.1 fL), thrombocytopenia (platelets 79×10⁹/L), indirect hyperbilirubinemia (1.3 mg/dL), markedly elevated lactate dehydrogenase (LDH 6500 IU/L), undetectable haptoglobin, and a low reticulocyte index (0.9). Peripheral smear showed very rare schistocytes (Figure 1). During her ED course, she developed an isolated fever to 103.5°F without infectious symptoms. Initial concern was for thrombotic microangiopathy (TMA), specifically thrombotic thrombocytopenic purpura (TTP). However, she was clinically well-appearing, unlike most patients with TTP, and workup revealed undetectable vitamin B12, raising the possibility of pseudo-TMA as an alternative diagnosis. Vitamin B12 supplementation was initiated at admission and led to rapid hematologic improvement and avoidance of plasmapheresis. Further workup revealed positive intrinsic factor and parietal cell antibodies, confirming pernicious anemia as the underlying etiology, with her lifelong vegetarian diet further exacerbating the deficiency.
Discussion: TTP is a medical emergency that requires rapid initiation of plasmapheresis, as it carries a 90% mortality rate when left untreated (1). However clinicians should bear in mind that, though rare, severe vitamin B12 deficiency can present with clinical and laboratory signs that mimic TTP, but key differences help distinguish them (2). In pseudo-TMA, macrocytosis is present and the reticulocyte index is low, reflecting ineffective erythropoiesis. Platelet counts are typically higher than in TTP, and bilirubin is only mildly elevated. LDH levels are often more markedly elevated in pseudo-TMA due to intramedullary hemolysis of LDH-rich nucleated erythroid precursor cells, whereas TTP primarily involves intravascular hemolysis of non-nucleated mature erythrocytes, which contain less LDH (3). In this case, pernicious anemia exacerbated by vegetarianism was determined to be the underlying cause of profound vitamin B12 deficiency. Pernicious anemia is an autoimmune disorder characterized by destruction of gastric parietal cells and loss of intrinsic factor, resulting in impaired vitamin B12 absorption and megaloblastic anemia (4). The patient’s lifelong vegetarian diet further exacerbated her risk, as vitamin B12 is found almost exclusively in animal-derived foods, and deficiency is common among vegetarians, especially lifelong adherents (5).
Conclusions: This case illustrates that very high LDH, low reticulocyte index, and macrocytosis in the setting of hemolytic anemia and thrombocytopenia should prompt consideration of pseudo-TMA from vitamin B12 deficiency, especially when supported by dietary and autoimmune risk factors (6). This distinction is critical, as plasmapheresis is not indicated and may expose patients to unnecessary risk (7). Another clinical teaching point is that fever is a recognized but under-appreciated manifestation of severe megaloblastic anemia, occurring in up to 40% of cases and typically resolving with vitamin therapy (8). In the absence of infectious symptoms, fever should be considered a potential presentation of severe B12 deficiency and included in the differential for fever of unknown origin.