Background: Clinicians are most likely to incorporate peer feedback (PF) from trusted colleagues (1,2). Despite PF’s impact on practice and outcomes, effective PF is challenging in healthcare (3). Many hospital medicine providers lack formal PF training, creating a skills gap. Workplace cultures often prioritize harmony over growth-oriented critique, making constructive criticism risky and resulting in missed development opportunities (4).
Purpose: We aimed to develop and implement the POISE communication framework to improve hospital medicine providers’ skills in giving and receiving both positive and constructive PF, with a focus on building trust and fostering a feedback-oriented, growth mindset culture.
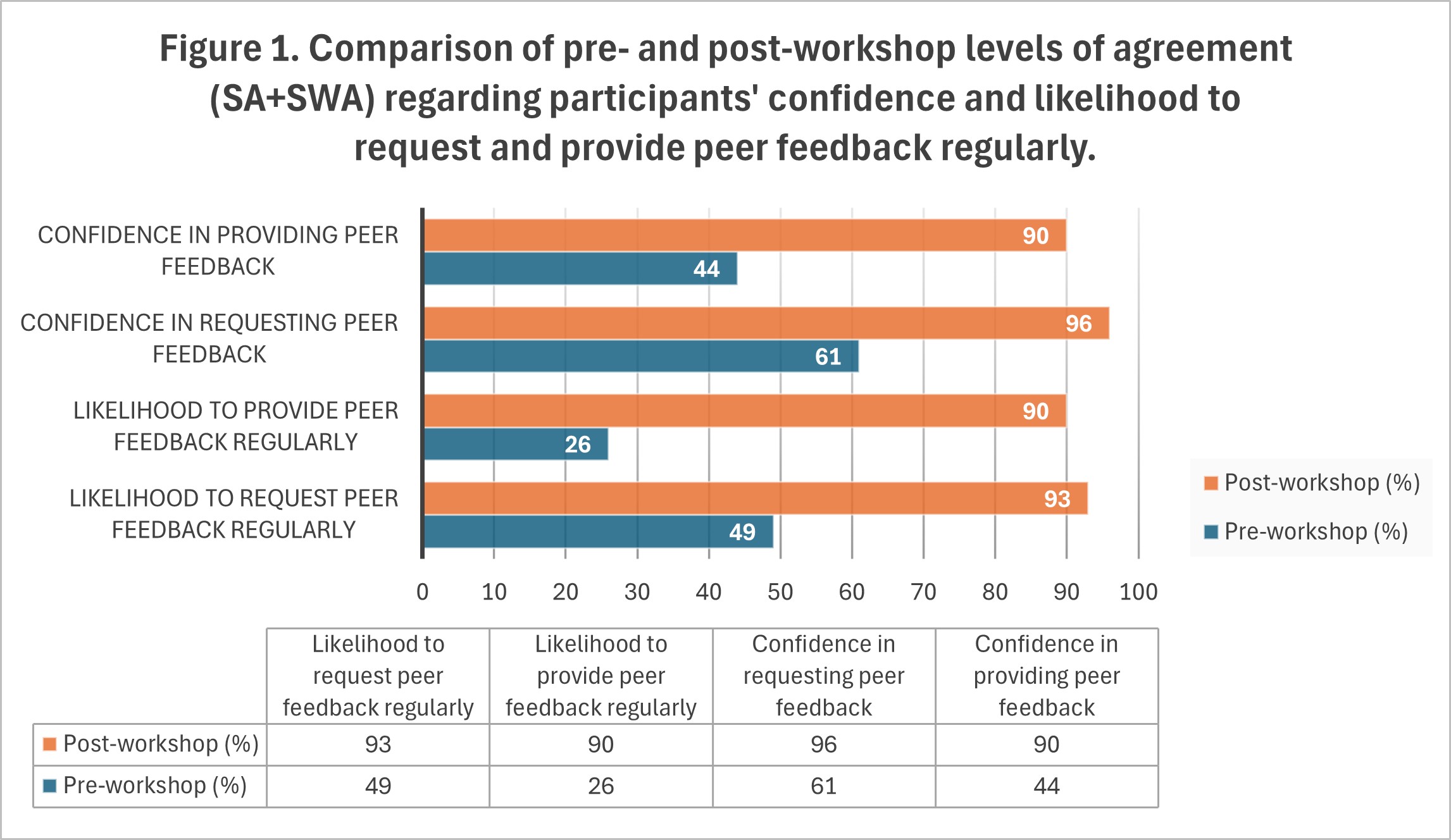
Description: An interactive workshop addressed the skill of PF among hospital medicine providers, using polling, scenario discussions, POISE framework introduction (see Table 1), demonstrations, and role-play in simulated clinical settings. The workshop was offered to clinicians in Hospital Medicine and Geriatrics at a single academic center. Pre- and post-workshop surveys used a 5-point Likert scale (Strongly Agree, SA; Somewhat Agree, SWA; Neither Agree nor Disagree, NAND; Somewhat Disagree, SWD; and Strongly Disagree, SD) to assess experience and confidence in PF. Twenty-eight participants (range: 1–28 years in practice) completed both surveys.Pre-workshop, only half regularly requested PF (SA: 12%, SWA: 37%, NAND: 27%, SWD: 16%, SD: 7%), and even fewer regularly provided it (SA+SWA: 26%, SWD+SD: 45%). PF exchange was infrequent: 42% sought PF at least monthly, while 40% asked less than 2–3 times/year or never; 31% provided PF less than 2–3 times/year. Most found PF easier when requested (SA+SWA: 88%) and preferred in-person exchange (receiving: 51%, giving: 57%). PF was universally regarded as important (SA+SWA >95%), but formal PF training was limited (42%), and few felt current feedback was sufficient (SA+SWA: 23%, NAND: 30%, SWD+SD: 47%). Major barriers included time constraints, awkwardness, power differentials, unclear expectations, and potential negative impact on relationships. Nonetheless, 89% had positive experiences receiving PF, 74% giving PF, and 94% reported changing practice due to feedback.Post-workshop surveys (see Figure 1) showed substantial increases in all domains: participants reported greater confidence and willingness to engage in PF, increased ability to recognize feedback opportunities (SA: 72%), and higher agreement for both giving and receiving PF. The POISE framework, role-play, and feedback timing strategies were considered the most useful workshop components.
Conclusions: A targeted PF workshop enhanced participants’ confidence and intent to engage in PF, providing practical tools for effective exchange. Results highlight the need for structured interventions to build PF culture among hospital-based teams. Continued work should integrate PF skills into clinical education and provide ongoing institutional support for regular, meaningful PF exchange.
.jpg)