Background: Mitral stenosis (MS) frequently coexists with atrial fibrillation (AF) and is known to precipitate or exacerbate heart failure with preserved ejection fraction (HFpEF). Whether MS confers additional short-term mortality risk in patients hospitalized with both HFpEF and AF has not been well characterized in contemporary U.S. cohort.
Methods: Using the 2018–2022 U.S. National Inpatient Sample, we identified adult hospitalizations with HFpEF as the principal diagnosis and comorbid AF. Mitral stenosis (rheumatic or non-rheumatic) was identified in any diagnostic position. Survey-weighted multivariable logistic regression examined the independent association of MS with in-hospital mortality, adjusting for age, sex, race, ZIP-code income quartile, Charlson comorbidity index, primary payer, hospital region, bed size, and location/teaching status.
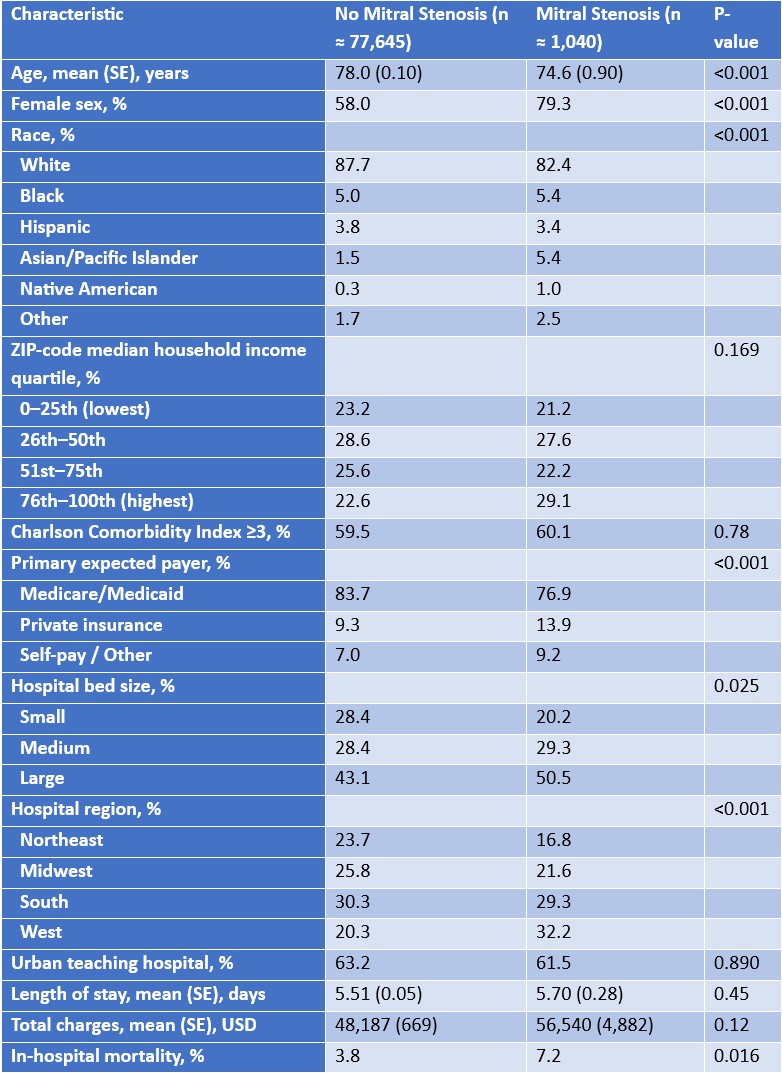
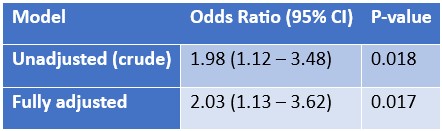
Results: Of an estimated 78,685 hospitalizations with HFpEF and AF, 1.3% (weighted n ≈ 1,040) had concomitant mitral stenosis. Patients with MS were younger (mean age 74.6 vs. 78.0 years), predominantly female (79.3% vs. 58.0%), and more often treated at large urban teaching hospitals and in the West (all P < 0.001). Crude in-hospital mortality was 7.2% in the MS group versus 3.8% in the non-MS group (P = 0.016). After comprehensive multivariable adjustment, MS remained independently associated with approximately doubled odds of in-hospital death (adjusted OR 2.03, 95% CI 1.13–3.62, P = 0.017). Additional independent predictors of mortality included older age (OR 1.04 per year, 95% CI 1.03–1.05), female sex (OR 1.30, 95% CI 1.09–1.55), and higher Charlson comorbidity index (OR 1.14, 95% CI 1.09–1.19). Mean total hospital charges were higher among patients with MS ($56,540 vs. $48,187), despite similar length of stay.
Conclusions: In a large, nationally representative cohort of patients hospitalized with HFpEF and atrial fibrillation, comorbid mitral stenosis affected 1.3% of cases and was independently associated with a twofold higher risk of in-hospital mortality despite a younger age and greater concentration in high-volume centers. These findings identify mitral stenosis as an important adverse prognostic marker in this population and support aggressive diagnostic evaluation and consideration of valve-directed therapies (percutaneous mitral balloon commissurotomy or surgery) to potentially improve outcomes in this high-risk subgroup.