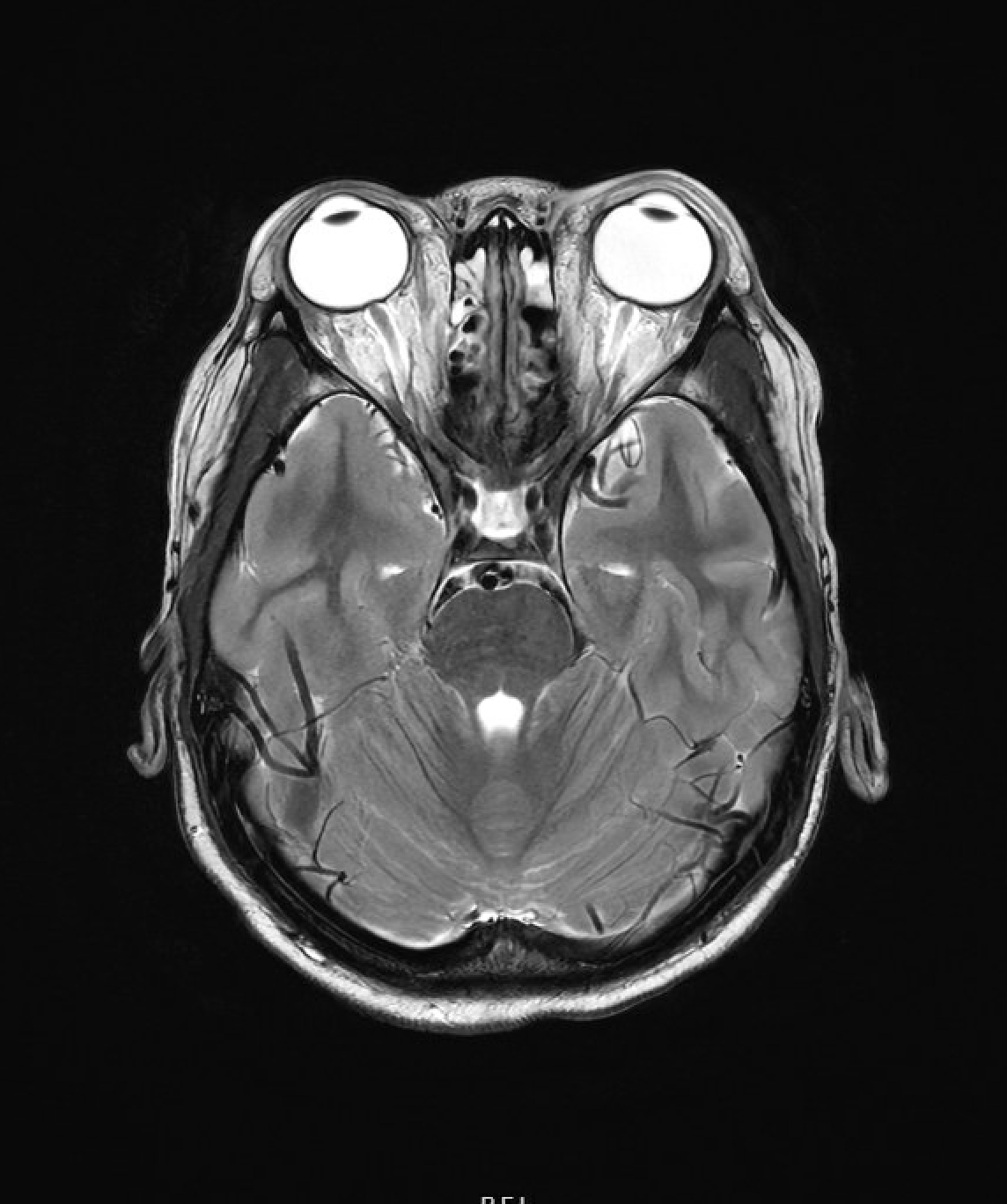
Case Presentation: A 9-year-old male with diagnosis of X-linked Lymphoproliferative Syndrome, undergoing stem cell transplant developed fevers, rash, nausea, positional headache, and lethargy three weeks after transplant. Neurological exam demonstrated grossly intact cranial nerve function, no clonus, and no further focal neurological deficits. His skin rash was characterized as diffuse coalescing erythematous papules and plaques covering face, trunk, and extremities. The differential included viral syndrome, meningitis, Graft versus Host Disease, Posterior Reversible Encephalopathy Syndrome, hemorrhage, or venous clot. MRI brain imaging remarkable for protrusion of the optic discs, proptosis of the bilateral globes, and narrowing of dural venous sinuses consistent with elevated intracranial pressure. He was started on antibiotics for bacterial meningitis given his immunocompromised state. A diagnostic and therapeutic lumbar puncture (LP) recorded an opening pressure of 48 cm H2O, nucleated cell count of 11x 10^6/L, RBC count 0, Protein 30 mg/dL, Glucose 53 mg/dL. The patient had improvement in headache and nausea after LP. Human herpesvirus 6 (HHV-6) CSF resulted positive with 2000 copies/mL, with HHV-6 serum resulting positive with 15756 copies/mL in the following days. The patient was diagnosed with acute HHV-6 encephalitis and started on treatment with ganciclovir and foscarnet. Antibiotics were quickly discontinued. After three weeks of antiviral treatment, a repeat LP demonstrated persistence of HHV-6, continued elevated opening pressure of 46 cm H2O. He remained on antiviral therapy serial LP three weeks following showed clearance of HHV-6 in the CSF.
Discussion: HHV-6 is best known for causing roseola infantum but has a broad range of manifestations including acute febrile illness without rash, febrile seizures, hepatitis, pneumonia, myocarditis, and meningoencephalitis. HHV-6 can have periods of latency after integrating into host cells’ telomeres and can be reactivated when patients are immunocompromised. HHV-6 reactivation typically occurs 2-6 weeks after bone marrow transplant. CNS involvement in patient undergoing transplant more often presents as altered consciousness, amnesia, seizures, and focal neurologic symptoms. When treatment is required, first line agents include ganciclovir and foscarnet, as single agents or in combination. Treatment length is for a minimum of three weeks and ultimately is determined by improvement in symptoms and HHV-6 DNA detectability.
Conclusions: Headaches and lethargy in a patient undergoing bone marrow transplant should immediately be worked up to rule out life-threatening illnesses, including HHV-6 CNS infection. Given that reactivation can occur up to 6 weeks post-transplant and the diversity of transplant service coverage, it is important for all pediatric hospitalists to recognize this syndrome.