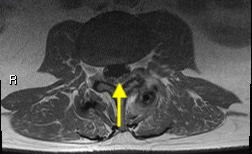
Case Presentation: A 50-year-old man without pertinent medical history presented with fever and confusion. He reported recent outdoor exposure in the Northeastern USA. Vital signs were significant for a fever of 39.4 °C (102.9 °F), heart rate of 71 bpm, normotension and eupnea. Physical exam was remarkable for an ill appearance, confusional state, and no nuchal rigidity/Kernig/Brudzinski. However, within 24 hours, he developed nuchal rigidity and difficulty following commands. Laboratory studies were remarkable for white blood cells 19.9 K/µL and lactate 3 mmol/L. Blood cultures were obtained, and he received empiric antibiotic treatment (vancomycin, ceftriaxone, ampicillin, doxycycline, and acyclovir) for suspected central nervous system infection. A lumbar puncture (LP) showed cerebrospinal fluid (CSF) with lymphocytic pleocytosis, elevated protein, and positive West Nile virus (WNV) IgM, confirming WNV encephalitis. He improved with supportive therapy. His hospital course was complicated by right facial flaccid paralysis on day 10, progressing to facial diplegia. Repeat LP revealed albuminocytologic dissociation, and lumbar (L) spine MRI demonstrated diffuse cauda equina enhancement at the L3-L4 level (figure 1-2), suggesting a Guillain–Barré syndrome (GBS) spectrum disorder. Neurology was consulted and electromyography was nondiagnostic. Intravenous immunoglobulin (IVIG) was initiated with subsequent neurological improvement.
Discussion: WNV is the leading cause of neuroinvasive arboviral disease in the USA, peaking in the summer and early fall. While focal neurologic deficits occur in < 1% of cases, with ~16% of those manifesting as cranial neuropathies (such as asymmetric flaccid paralysis), facial diplegia is rare. Patients mostly affected are older and immunocompromised. WNV neurotropism can mimic or trigger immune-mediated neuropathies such as GBS. This association of WNV and GBS is estimated at 0.6 per 100,000 cases annually. Distinguishing between direct viral anterior horn cell injury (in acute flaccid paralysis) and post-infectious demyelination (in GBS) is clinically challenging. In early GBS, nerve conduction studies may appear normal; therefore, nerve-root enhancement on MRI and albuminocytologic dissociation in CSF are diagnostic. IVIG remains the standard of care. Corticosteroids lack benefit in classic GBS, and their role in WNV encephalitis remains uncertain. With an aging population and ecological conditions favorable to mosquito-borne transmission, we may see rising cases of WNV-associated neurologic complications in the future. Prompt recognition is crucial for improved patient outcomes.
Conclusions: This case underscores the overlap between viral neuroinvasive disease and immune-mediated neuropathy. In patients recovering from WNV encephalitis who develop new delayed focal neurologic deficits, clinicians should maintain a high index of suspicion for GBS. Early MRI and CSF evaluation can establish the diagnosis, even when initial nerve conduction studies are inconclusive, enabling timely immunotherapy and improved prognosis.