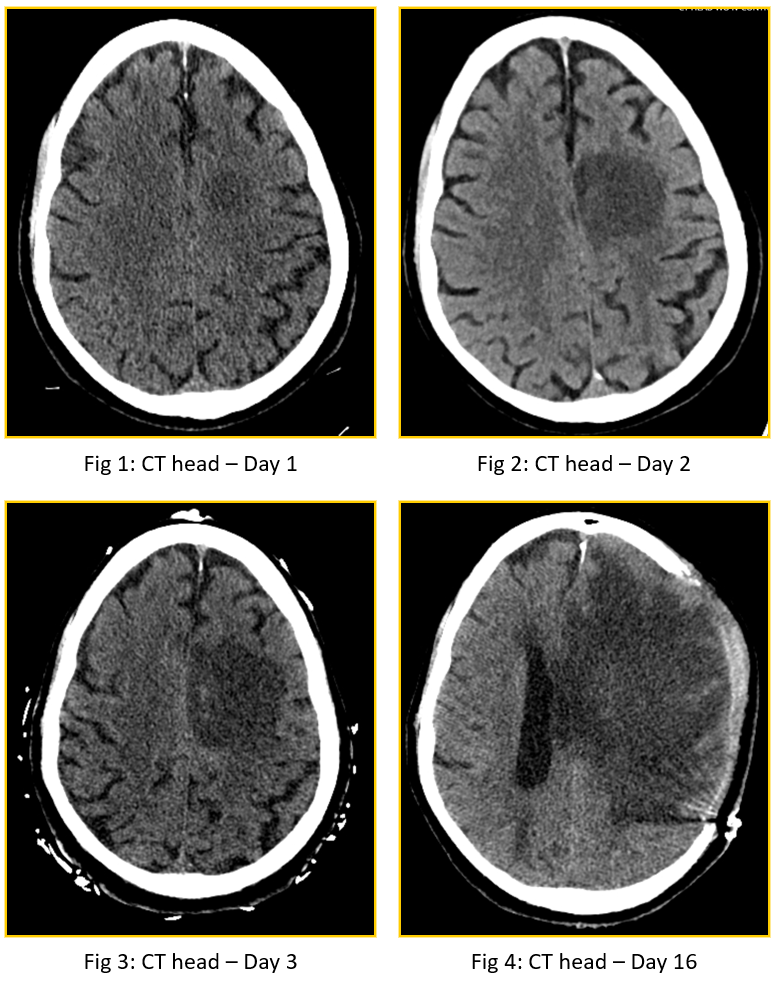
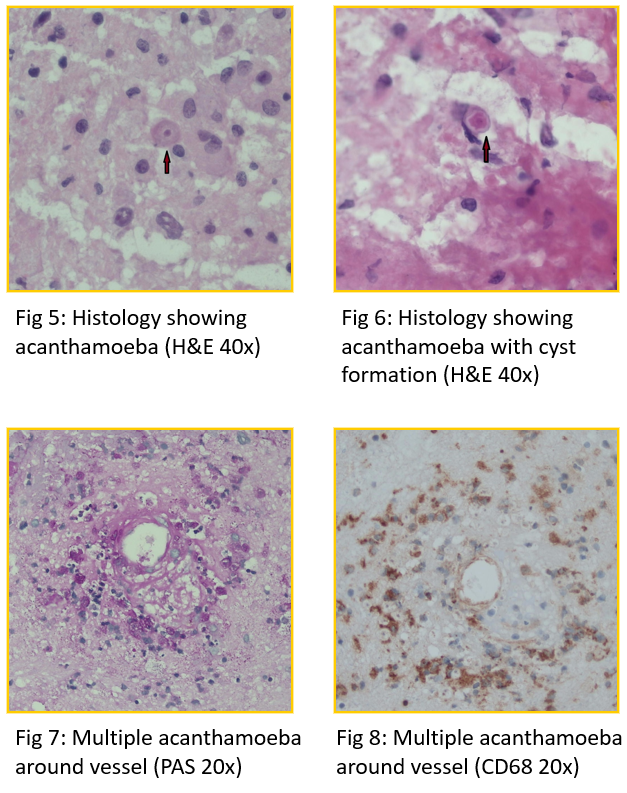
Case Presentation: Acanthamoeba spp. are one of three pathogenic free-living amebae that are known to cause rare but severe infections including usually fatal meningoencephalits1. We present a case of Acanthamoeba encephalitis in an immunocompromised patient. A 71-year-old male, with known chronic lymphocytic leukemia (CLL), on ibrutinib, was admitted with fevers, mild expressive aphasia, and right arm weakness. Initial non-contrast CT head revealed a round left frontal lobe lesion that was concerning for ischemic stroke with abscess being a less likely possibility. Guideline based stroke work-up was initiated. He was also started on IV Ampicillin, IV Ceftriaxone and IV Vancomycin, due to the possibility of meningoencephalitis, while MRI brain was pending. Over the next 24 hours, the patient became less responsive and right sided weakness worsened. MRI brain and repeat CT head showed enlarging left frontal lobe lesion with surrounding vasogenic edema concerning for infectious process. He was moved to the Neurology ICU and anti-infective therapy was broadened to include IV Isavuconazole to cover fungal infections. CSF studies were sent and showed slightly elevated protein. CSF microscopy and culture were negative. Extensive work-up for CNS infections was also negative. He continued to deteriorate clinically with further enlargement of CNS lesion on CT head. Subsequently, he underwent a decompressive craniectomy and biopsy of the CNS lesion. Intra-operative frozen section was unrevealing. With continuing clinical deterioration, the patient was placed on mechanical ventilation. IV Amphotericin B was also added. Three days later his pathology results revealed that he had amebic encephalitis. He was started on Azithromycin, Sulfadiazine, Flucytosine, Fluconazole and Miltefosine. Tissue samples were sent to the Centers for Disease Control (CDC) and they helped confirm the diagnosis of Acanthamoeba encephalitis. Despite the recommended treatment, the patient did not improve. Following discussions with family, the patient was transferred to hospice after two weeks where he died.
Discussion: Acanthamoeba is one of three amebae that are known to cause disease in humans. These include granulomatous encephalitis, keratitis and cutaneous infections.2 Acanthamoeba encephalitis has an extremely high mortality rate of 94 percent in USA.1 While infections are rare and typically occur in immunocompromised patients, they are increasing in frequency with increased use of immunomodulators.3 There is one other reported case from the US of a patient with CLL, on ibrutinib, who developed granulomatous acanthamoeba encephalitis.4 However, our patient was unique because his disease was rapidly progressive and granulomas were not identified on biopsy unlike the majority of Acanthamoeba cases.
Conclusions: Given the rise of immunomodulator use, Acanthamoeba encephalitis should be considered as a possible diagnosis in immunocompromised patients with systemic signs of infection and progressive neurological symptoms.