Background: Telemedicine emerged as an innovative approach to addressing staffing shortages for hospitalists in resource-limited areas (1), the COVID-19 surge (2), and off-hour shifts (3). Telemedicine can be adapted to non-traditional hospitalist roles, i.e. the triagist where a hospitalist assesses patients for potential admissions and supports outpatient to inpatient transitions (4). Modifying the triagist to a remote or off-site model may increase scheduling flexibility and work-life balance for hospitalists.
Purpose: We sought to adapt the night triage shift (NTr) for remote work and explore the feasibility of a remote triage model by assessing physician satisfaction with working as and working with a remote triagist.
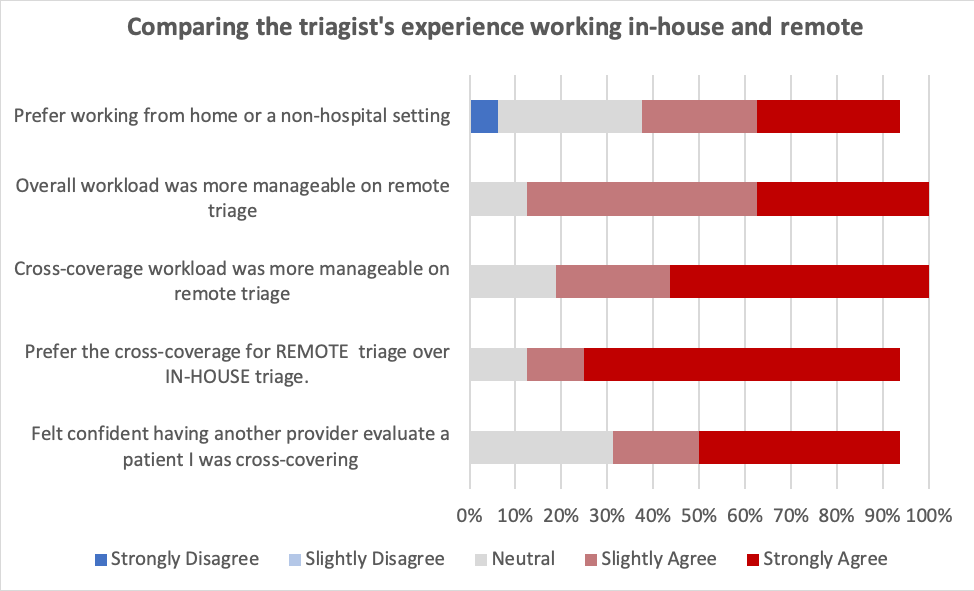
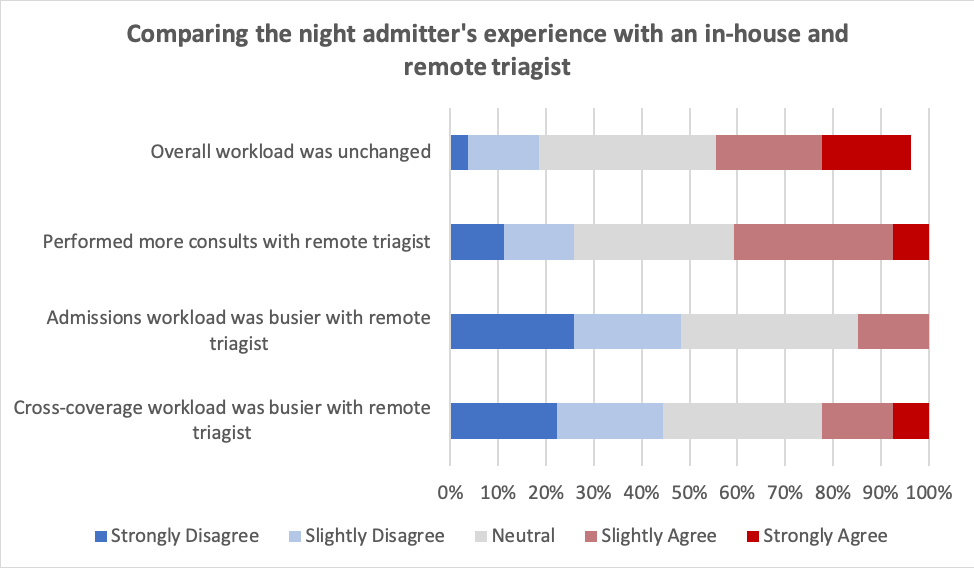
Description: We altered a 12-hour hospitalist NTr at a large academic center from traditional in-house coverage to a remote shift. NTr responsibilities of managing admissions, transfers, and patient distribution remained consistent with the pre-intervention role, but remote NTr cross-coverage assignment was altered to a lower acuity cohort. The additional 4 in-house night providers (N1-4) maintained admitting and cross-coverage responsibilities with N1 providing in-person evaluations for remote NTr cross-cover patients and N1-4 staffing new consults. Remote NTr accessed the electronic medical record via a virtual private network and communicated with N1-4 via text paging and telephone. Providers accessed electronic admission logs via a HIPAA-compliant data cloud. The pilot was implemented in June 2022 as a simulated remote experience with NTr in-house (weeks 1-3), then off-site (4.5 months). We then surveyed hospitalists who worked either triage or night shifts on their experience with an in-house vs remote triagist. Multiple choice, 5-point Likert scale, and open-ended questions were employed to assess perceptions of workload, patient safety, and work setting/interruptions. Qualitative analysis of write-in answers was reviewed and coded into themes within a priori domains.Of the 57 hospitalists surveyed, 27 responded (47.4%). Respondents reported working 3 or more night shifts a month (41%) and 3 or more triage shifts a month (35%). Of the respondents who work triage shifts (n=16), the majority preferred working remotely and agreed that overall workload and cross-coverage workload were more manageable on remote shifts [Fig. 1]. Technological or environmental issues were reported “never” or “rarely” encountered while working remotely by 87.5% of respondents. The majority of respondents on night shifts reported performing more consults with a remote NTr but disputed that cross-coverage or overall workload was busier [Fig. 2]. Safety concerns with a remote NTr were reported by 18.5% of respondents. Qualitative analysis in the domain of Triage Should not Cross-Cover Remotely identified themes of (1) delays in care, (2) communication issues, (3) busier workload for N1-4, and (4) safety concerns. In the Triage Should Work Remotely domain, comments centered around the theme that working remotely is doable and preferred.
Conclusions: In this feasibility pilot of remote NTr, we identified a preference for remote work by triagists. Technology was not reported as a barrier, but remote cross-coverage was a safety concern. Future iterations may need to account for other cross-coverage models and include clinical outcome analysis (i.e. safety events, time to first orders) and longitudinal assessment of physician burnout.