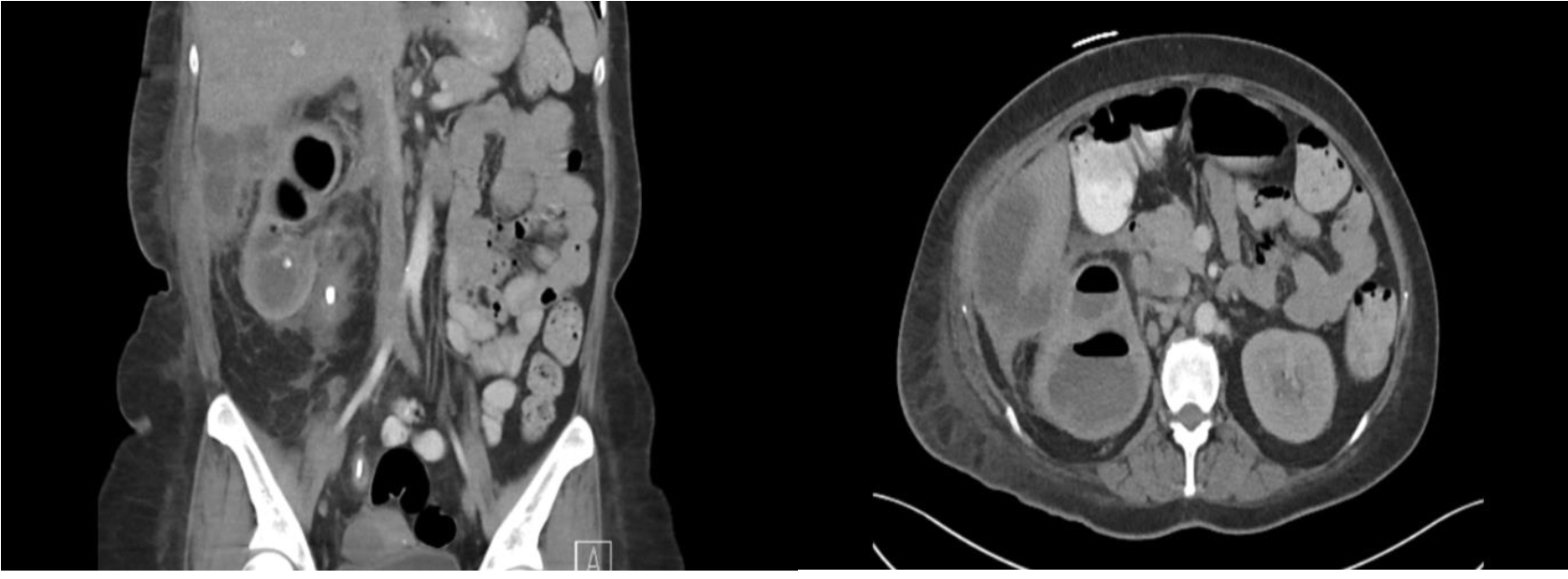
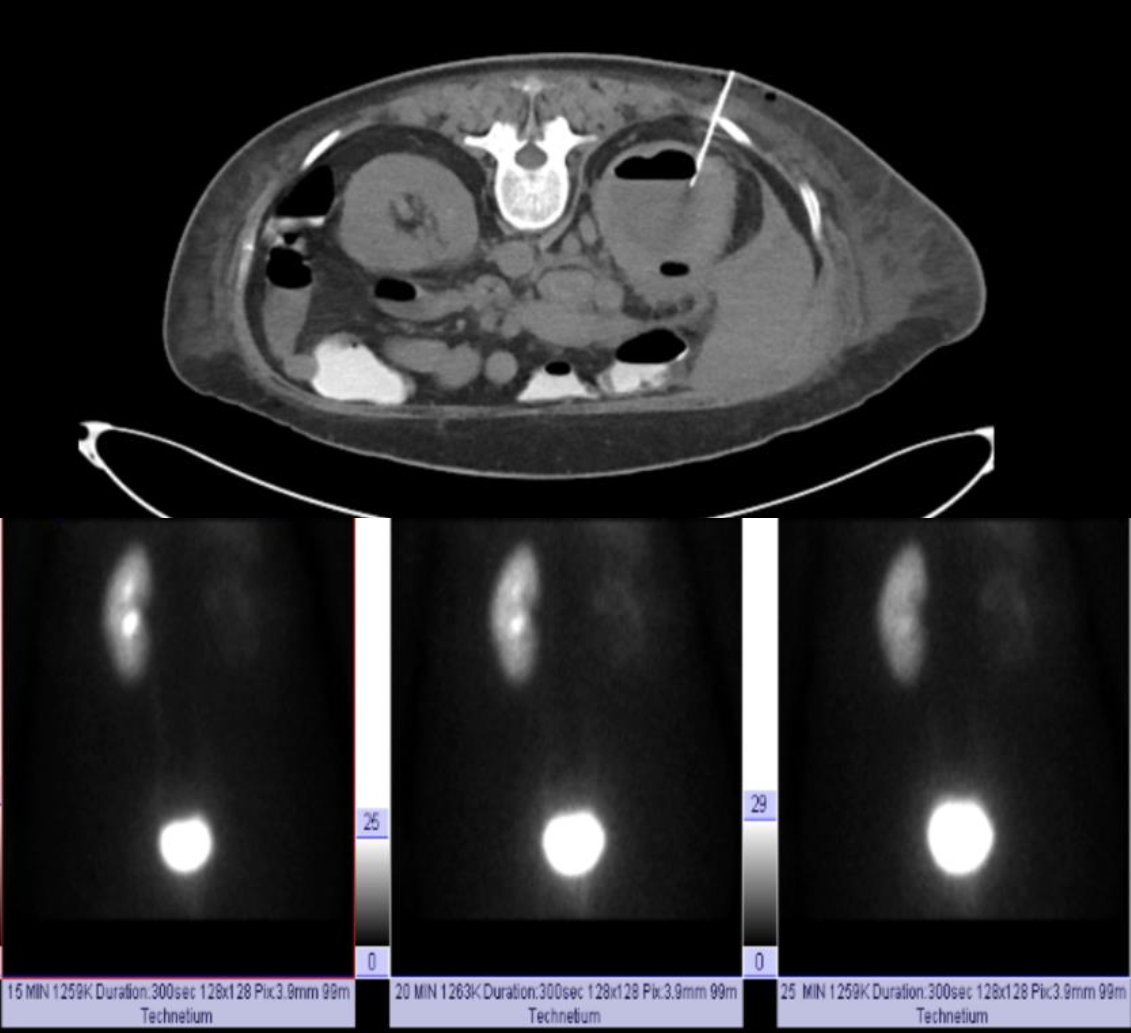
Case Presentation: A 41-year-old woman with a history of nephrolithiasis managed conservatively presented to the hospital with right flank and right upper quadrant pain. The pain initially started four months prior to her presentation, cramping in nature, rated 10/10 in intensity, intermittent, progressively worsening, initially well managed with ibuprofen, aggravated by movement, and relieved partially with rest. She had associated decreased appetite, weight loss of forty pounds over the past four months, and dyspnea on exertion. Her temperature was 99.7 degrees Fahrenheit, heart rate 139bpm, blood pressure 100/71 mmHg, respiratory rate of 18 per minute and saturating 100% on room air. Physical examination was significant for, distress, right upper quadrant pain with a palpable liver, and right costovertebral angle tenderness. Admission labs were significant for WBC 10.53K/uL, Hb 5.9 g/dL, HCT 22.8%, Platelets 644 K/uL, and an unremarkable metabolic panel. CT abdomen/pelvis with contrast revealed a right-sided staghorn calculus and an abscess of 7.3 x 5.7 cm within the right kidney extending to the right colon connecting to an abscess within the liver of 9 x 3.8 cm (Figures 1 and 2). The patient was initiated on piperacillin-tazobactam and underwent a fluid aspiration of hepatic abscess and drain placement (Figure 3). Cultures of the body fluid and urine culture showed heavy growth of E. coli. The patient was discharged with a 4-week course of Levofloxacin with the drain in place and scheduled for a right nephrectomy after a nuclear medicine Kidney with flow and function test showed a nonfunctioning right kidney (Figure 4).
Discussion: Xanthogranulomatous Pyelonephritis (XGP) is a rare sequela of chronic pyelonephritis involving the destruction of normal renal tissue with nonfunctioning granulomatous infiltration. XGP can extend into other solid organ structures, such as the liver or colon, causing extensive abscesses. XGP represents less than 1% of the cases of pyelonephritis, and only a few case reports of these abscesses extending into the gastrointestinal tract exist in literature. We present a rare case of XGP with the abscess extension into the colon and liver.
Conclusions: XGP is a rare complication of chronic pyelonephritis, with renal infections and obstruction as common etiologies. As they represent less than 1% of cases of chronic pyelonephritis, they may or may not be suspected on initial physical examination, making imaging crucial in diagnosis. The abscess typically grows E. coli, Klebsiella, or Proteus sp., which can extend alarmingly into multiple organs. The prognosis for XGP is excellent with prompt management consisting of antibiotics to control the infection and surgical intervention to remove the affected tissue. A multidisciplinary approach is required to prevent permanent complications such as loss of renal function as observed in this case. In patients with abscesses involving both the genitourinary system and gastrointestinal tract, XGP should remain high on the differential.