Background: Large Language Models (LLMs) and Artificial Intelligence (AI) tools are rapidly permeating clinical workflows. While adoption is accelerating, the specific patterns of usage, trust levels, and impact on clinical decision-making among trainees remain under-characterized. This study evaluates the current landscape of AI integration within a community-based Internal Medicine Residency Program to identify usage trends and curricular needs.
Methods: A cross-sectional survey was administered to Internal Medicine residents (PGY-1 through PGY-3) at Griffin Hospital. The survey instrument assessed demographic data, pre-residency familiarity with AI, current adoption rates, and specific platforms utilized. Key domains of inquiry included the impact of AI on diagnostic accuracy, differential diagnosis generation, and treatment personalization. Additionally, the survey evaluated residents’ habits regarding the verification of AI data, their confidence in AI explainability, perceived biases, and the quantitative impact on administrative burden versus patient care time.
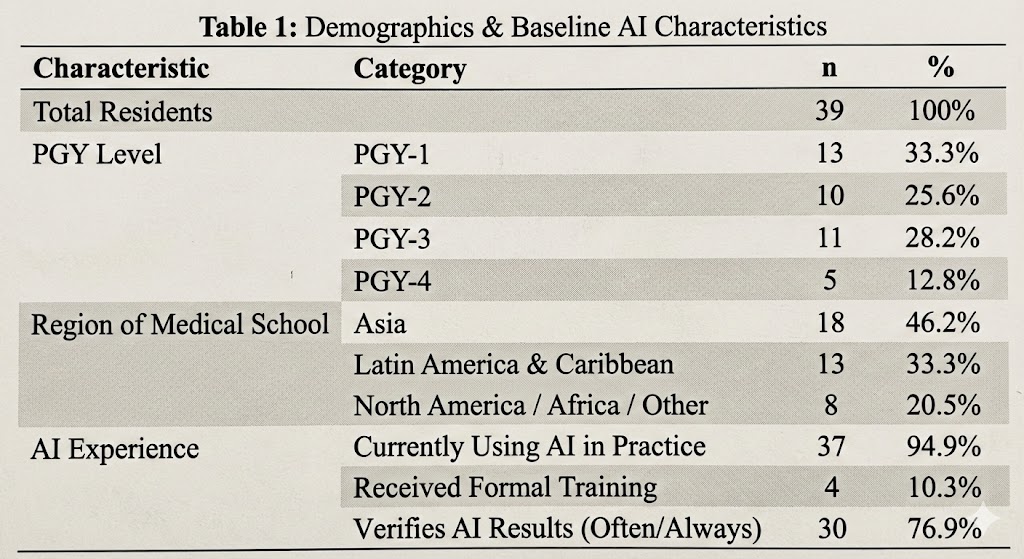
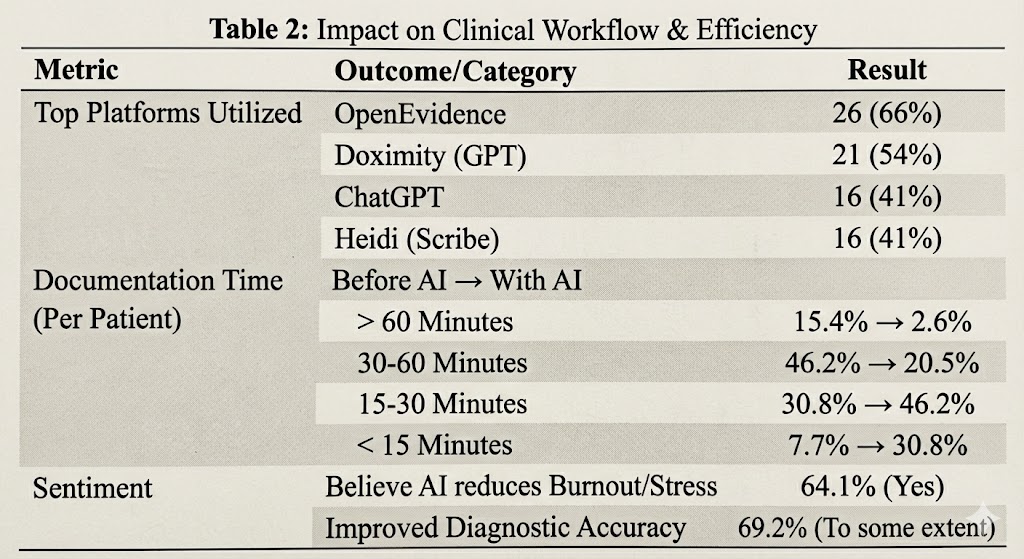
Results: Respondents reflected a diverse demographic distribution across postgraduate years and geographic origins.Adoption vs. Education: There is a significant discordance between usage and training. While a majority of residents actively utilize AI tools (predominantly LLMs) for medical practice, formal institutional training is virtually absent. Skill acquisition is primarily driven by self-study and peer learning.Clinical Utility: Residents reported utilizing AI to broaden differential diagnoses, summarize complex medical literature, and streamline documentation. A notable finding was the reported reduction in time spent on administrative tasks (ranging from 15 to 60 minutes daily), which residents correlated with increased availability for direct patient care.Trust and Verification: Despite high usage, blind reliance is low. Residents frequently verify AI-generated recommendations against traditional medical guidelines and literature, citing concerns over “hallucinations,” bias, and accuracy.Sentiment: Qualitative feedback revealed a duality in resident sentiment: while AI is viewed as a vital tool for efficiency and “survival” in modern practice, there are prevailing concerns regarding potential dependency, data privacy, and the fear that AI-driven efficiency may paradoxically lead to increased workload expectations.
Conclusions: AI has organically integrated into the residency workflow at Griffin Hospital, serving as a potent adjunct for clinical reasoning and administrative efficiency. However, the reliance on informal self-training highlights a critical gap in Graduate Medical Education (GME). To ensure patient safety and maximize utility, residency programs must formalize AI curricula that focus on prompt engineering, understanding algorithmic limitations, and verifying outputs, transitioning AI from a novel convenience to a rigorously managed clinical tool.