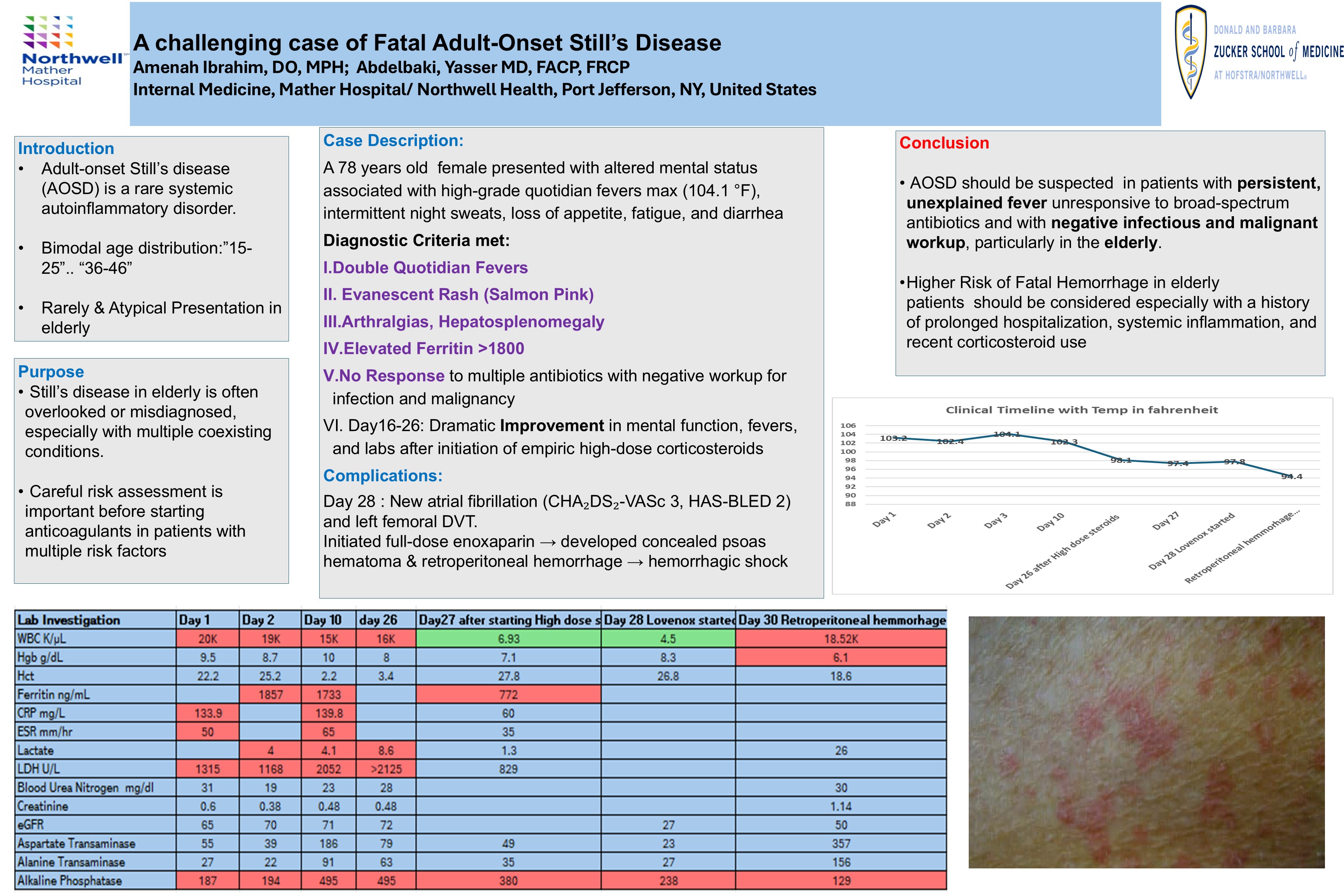
Case Presentation: Purpose: -To highlight differentiating AOSD from sepsis and systemic inflammatory response syndromes (SIRS) in elderly patients with confounding, complex, comorbidities. -To remind clinicians that when appropriate anticoagulation is initiated for two new unrelated comorbidities, retroperitoneal hemorrhage may be massive and lead to fatal shock.Case description: An elderly female presented with high-grade quotidian fevers (103.2°F), leukocytosis (20K), anemia (Hgb 9.5), hypercalcemia (Ca 11.5), with normal renal and Liver function tests inflammatory markers were markedly elevated including ferritin (1857 ng/mL), CRP (74 mg/L), ESR (62 mm/hr.), and LDH (1315 U/L), without an M-spike . Despite empiric broad-spectrum antibiotics, she remained febrile with progressive lethargy (see Timeline fever). Initial extensive Infectious workup was negative. Autoimmune and malignancy workups revealed an elevated ANA and questionable low-grade CLL/SLL on bone marrow biopsy, but rheumatology thought history, physical and exam and other negative serologies ruled out SLE, extensive imaging evaluation, which revealed mild splenomegaly. Persistently elevated inflammatory markers, double quotidian fevers, evanescent rash, and arthralgias supported a possible diagnosis of adult-onset Still’s disease (AOSD) and empiric high-dose corticosteroids led to improvement in clinical and laboratory parameters. However, on her fifth day of steroid therapy, hospital day 27 and just prior to a planned discharge, she developed new-onset atrial fibrillation with RVR, and a left femoral DVT. Anticoagulation with full-dose enoxaparin was initiated that led to a retroperitoneal hemorrhage from a hidden psoas hematoma, causing hemorrhagic shock and death despite emergent blood transfusion and IR embolization.
Discussion: AOSD in elderly patients often presents atypically and mimics sepsis or malignancy, leading to delayed diagnosis. Steroid responsiveness can help support diagnosis once infectious and autoimmune etiologies are excluded. This case also underscores that anticoagulation, while guideline-driven for atrial fibrillation and DVT may pose catastrophic bleeding risks in frail, inflamed patients, especially when initiated during high-dose steroid therapy.
Conclusions: Our case demonstrates two important teaching moments: 1. A possible diagnosis of AOSD is challenging in an elderly patient with confounding comorbidities due to its nonspecific presentation and overlap with sepsis, malignancy, and other inflammatory or autoimmune conditions. Although AOSD typically presents in younger adults, cases in older individuals have been increasingly recognized, often with atypical features and longer diagnostic delays. 2. While anticoagulation is essential for stroke and thromboembolism prevention, particularly in the setting of DVT and high CHA₂DS₂-VASc scores, it may carry significant bleeding risk such as RP bleeding, perhaps exacerbated in the context of systemic inflammation, steroid use, or frailty.’