Background: Each year, tens of thousands of Americans seek emergency care for rectal bleeding, making hematochezia one of the most common gastrointestinal (GI) bleeding presentations (20–36 cases per 100,000 persons annually)1. In adults aged 18–44, most cases arise from benign anorectal sources, though inflammatory bowel disease (IBD) and diverticular disease remain relevant2. Despite overall low risk of malignancy or major hemorrhage, emergency department (ED) evaluation frequently leads to extensive testing, repeated visits, and inconsistent colonoscopy use. This study examines the inpatient admissions, diagnostic trends, and healthcare utilization patterns among adults aged 18–44 presenting with first-time hematochezia.
Methods: A retrospective cohort study using the TriNetX Research Network identified adults with a first ED diagnosis of hematochezia over the past 20 years. Patients with prior colorectal cancer or colorectal surgery were excluded. A total of 81,943 patients met criteria. The index event was the initial ED encounter for hematochezia, with outcomes tracked for 365 days. Clinical outcomes, healthcare utilization, and mortality were measured, and clinical characteristics were compared between admitted and non-admitted patients.
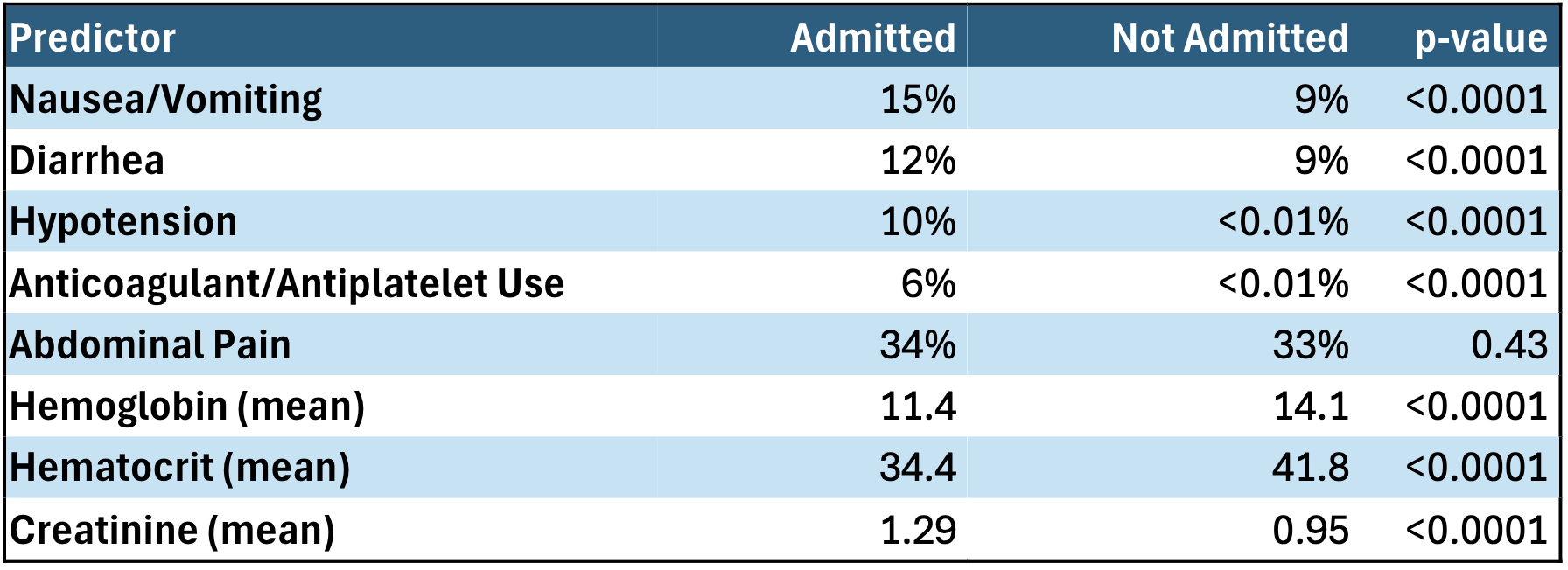
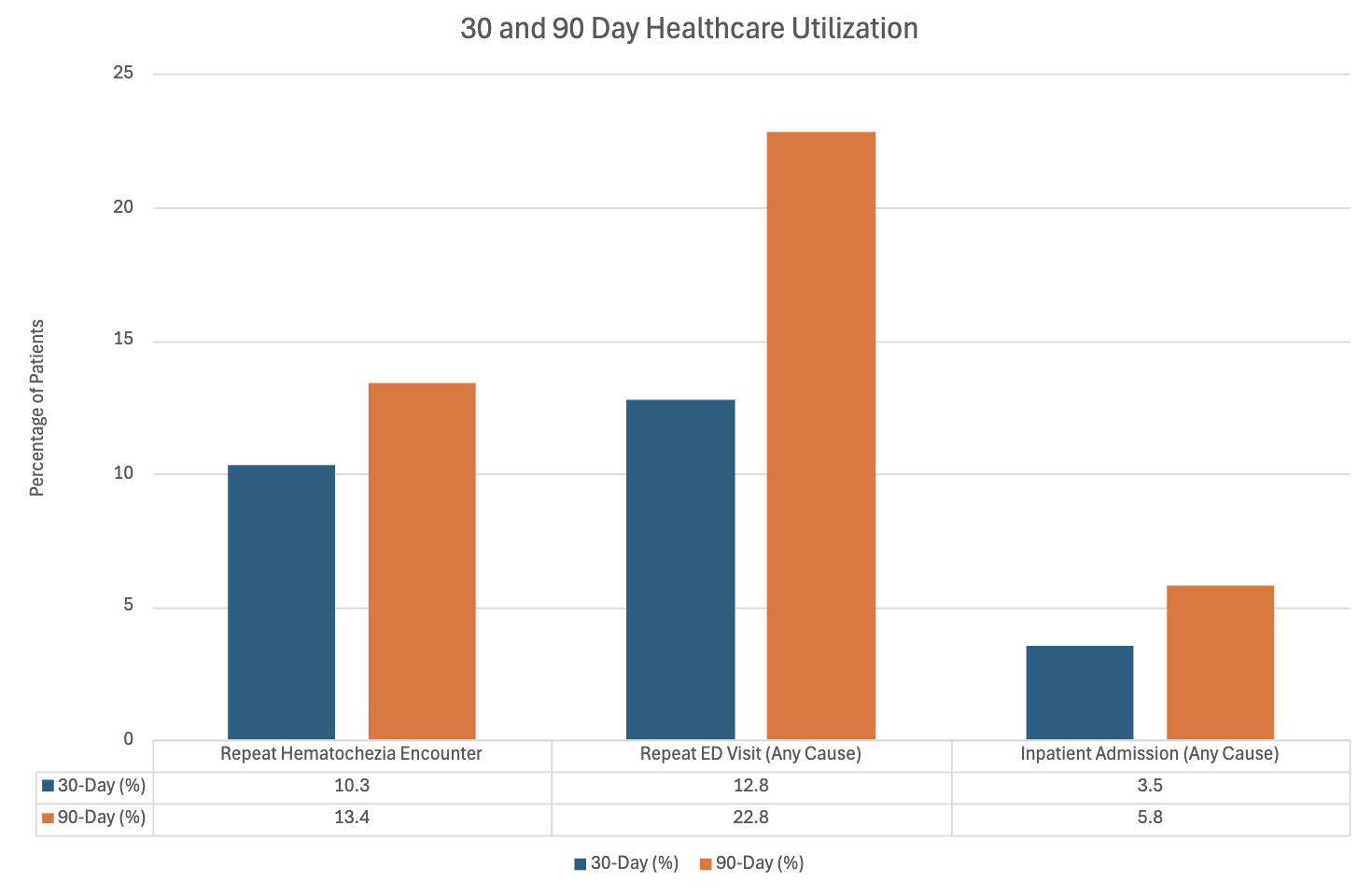
Results: Within one year of initial presentation, the most common new diagnoses were hemorrhoids (25.3%), anal fissures (4.7%), IBD (1.6%), diverticular disease (3.2%), malignancy (0.03%), and all-cause mortality (0.53%). A total of 3.4% of patients were admitted during the index ED visit. When comparing admitted with non-admitted patients, those admitted more often presented with nausea/vomiting (15% vs 9%), diarrhea (12% vs 9%), hypotension (10% vs < 0.01%), and anticoagulant/antiplatelet use (6% vs < 0.01%) (all p< 0.0001). There was no significant difference in abdominal pain (34% vs 33%; p=0.43). Admitted patients had lower mean hemoglobin/hematocrit (11.4 vs 14.1; 34.4 vs 41.8), and higher mean creatinine (1.29 vs 0.95) (all p< 0.0001). Among admitted patients, mean length of stay was 4.9 days (median 2 days), and one-year all-cause mortality was 7.3%. Repeat hematochezia encounters occurred in 10.3% at 30 days and 13.4% at 90 days, ED visits for any cause in 12.8% at 30 days and 22.8% at 90 days, and inpatient admissions in 3.5% at 30 days and 5.8% at 90 days. Colonoscopy or sigmoidoscopy was performed in 4.7% of patients at 30 days, 9.5% at 6 months, and 10.6% at one year. Early colonoscopy (< 30 days) was more common in White and male patients, while Black and Hispanic patients had lower rates.
Conclusions: The predominance of benign anorectal conditions among young adults presenting with hematochezia underscores the generally low likelihood of serious disease in this group. However, the presence of clinically significant conditions such as IBD, diverticular disease, and malignancy remains a serious concern. During ED triage, certain clinical symptoms may provide more diagnostic value (Nausea/vomiting, hypotension, anemia, AKI), compared to others such as abdominal pain. Establishing clear criteria for inpatient admission and ED triage, and consistent outpatient follow-up is crucial to prevent missed diagnoses while reducing repeat visits. Limited colonoscopy utilization (< 11% at 1 year) highlights the ongoing uncertainty in selecting which patients warrant endoscopy. Despite broad, multi-institution representation, the retrospective design and reliance on diagnostic coding introduces potential for residual confounding.