
Background: Ischemic colitis is a rapidly progressive gastrointestinal emergency that causes acute abdominal pain, inflammation, and potentially life-threatening bowel injury. Many mild cases resolve without intervention, but severe disease can quickly advance to necrosis, sepsis, or organ failure1. Ischemic colitis is correctly identified at presentation in only ~9% of patients and occurs at an incidence of 22.9 per 100,000, with higher risk in older adults, men, and those with atherosclerotic disease2. Although epidemiology and risk factors are described in literature, the early clinical course remains poorly characterized. Key uncertainties include the timing of imaging and endoscopy, early complication rates, surgical needs, and short-term mortality. This study evaluates diagnostic patterns, complications, and healthcare utilization following an initial inpatient diagnosis of ischemic colitis.
Methods: A multicenter retrospective cohort study was conducted using the TriNetX Research Network, identifying adults ≥18 years hospitalized with a first diagnosis of ischemic colitis. Patients with radiation proctitis, C. difficile colitis, infectious colitis, ulcerative colitis, or Crohn’s disease were excluded. A total of 8,113 patients met inclusion criteria. The index event was the initial inpatient encounter, with outcomes assessed across fixed intervals including 0–3 days (Computed tomography (CT), endoscopy, antibiotic use), 0–14 days (CT, endoscopy, antibiotics, colectomy, ostomy, transfusion, severe sepsis/shock, intensive care unit (ICU) admission, perforation/peritonitis), and mortality at 14, 30, and 90 days. Repeat emergency department (ED) and inpatient visits were measured at 15–30 and 30–90 days. Risk estimates reflected percentage frequencies generated within TriNetX.
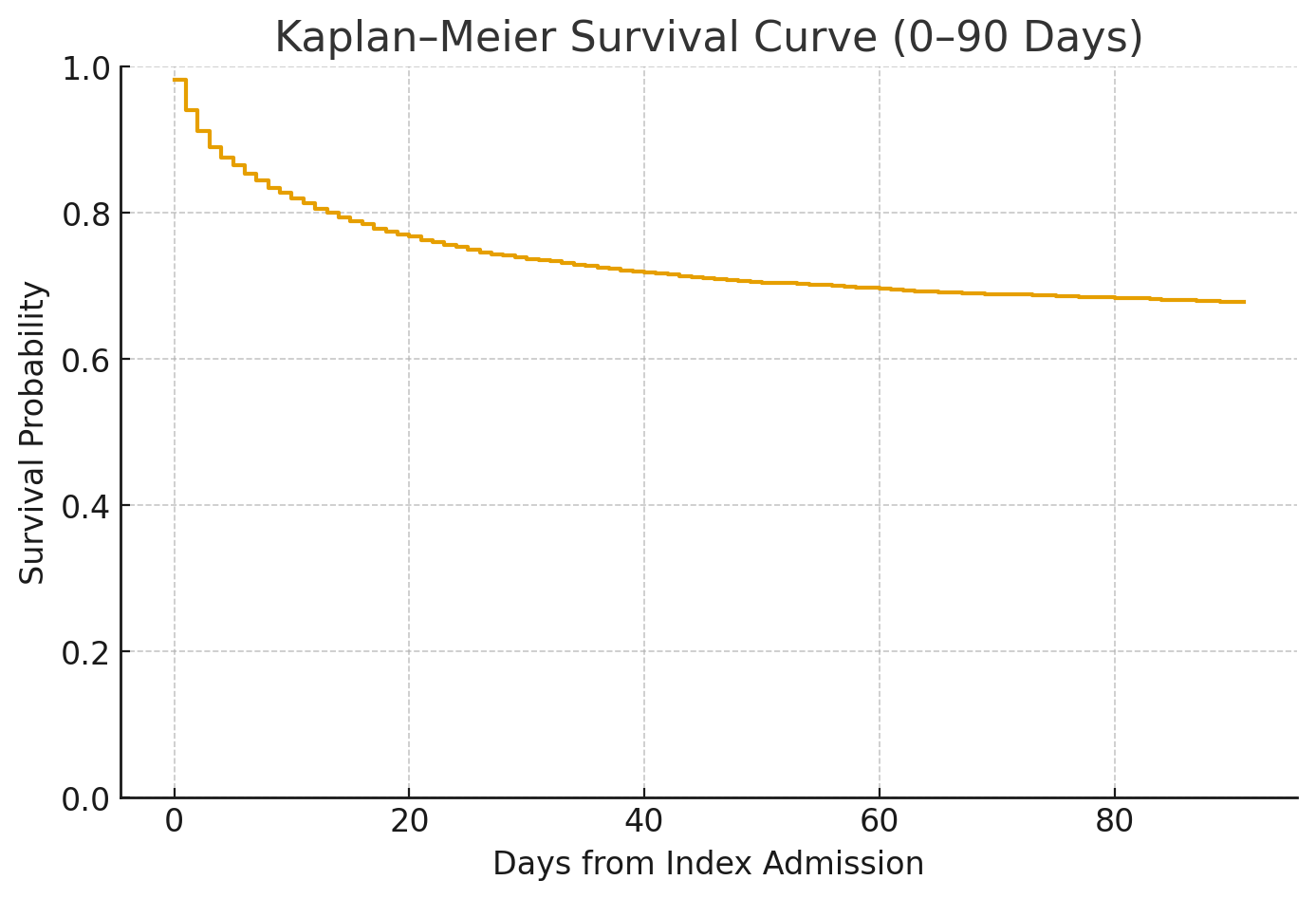
Results: Early clinical management is imperative. Within 3 days of diagnosis, 56.9% underwent CT imaging, 10.2% received colonoscopy or sigmoidoscopy, and 75.5% were treated with antibiotics. By 14 days, diagnostic and therapeutic interventions increased, with CT in 68.2%, endoscopy in 13.8%, and antibiotics in 84.8%. Severe complications by 14 days were frequent, including colectomy (28.1%), ostomy creation (19.6%), blood transfusion (15.2%), severe sepsis or shock (36.1%), ICU admission (48.1%), and perforation or peritonitis (32.8%). 14-day mortality reached 20.1%. Mortality continued to rise over time, with 30-day and 90-day mortality of 25.2% and 30.1%, respectively. Hospital utilization after the acute episode remained high: ED visits occurred in 4.5% of patients at 15–30 days and 9.9% at 30–90 days, while inpatient readmissions occurred in17.3% and 17.5% over the same intervals. The median length of stay following the initial diagnosis was 2 days (mean 4.6).
Conclusions: Hospitalized adults with ischemic colitis experienced substantial early morbidity, with high rates of sepsis, transfusion, surgical intervention, and nearly one in five patients dying within 14 days. Mortality continued to rise through 30 and 90 days, and both repeat ED visits and inpatient readmissions were frequent. These findings indicate that ischemic colitis carries a far more serious short-term course than often appreciated and requires close inpatient monitoring and structured follow-up after discharge. The multi-institution results likely extend to a broad inpatient population. However, reliance on coded data and absence of symptom severity or radiographic features remain important limitations.
.png)