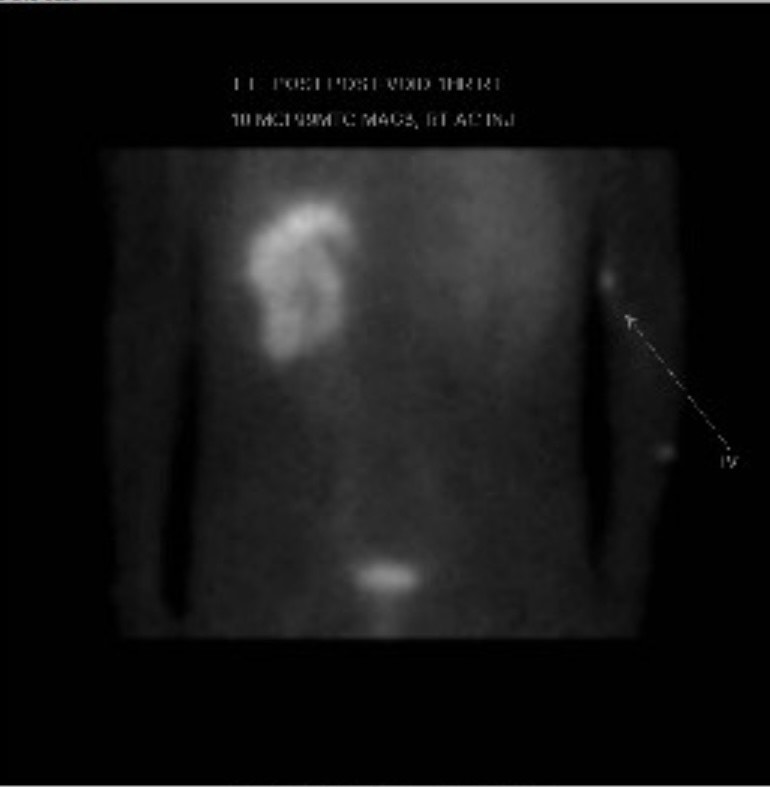
Case Presentation: A 43-year-old male from Guatemala with a history of alcohol abuse, brief incarceration and nephrolithiasis presented to the emergency room with abdominal pain and bloody diarrhea. He was found to have a psoas abscess and subsequently underwent radiologic aspiration and drainage of the lesion. Given the unusual intraosseous features on imaging, the patient was suspected to have spinal tuberculosis. Disseminated tuberculosis was confirmed through bilateral miliary pulmonary nodules on CT imaging, as well as subsequent bone marrow biopsy. Patient was also found to have acute kidney injury, with initial creatinine of 4.9 mg/dL and GFR of 13 ml/min. Patient subsequently had a CT abdomen and pelvis without contrast which demonstrated bilateral non-obstructing stones, moderate right hydronephrosis with atrophy and mild hydronephrosis on the left kidney. MRI brain showed multiple enhancing lesions indicative of multifocal tuberculomas, and the patient was started on dexamethasone with a planned taper. Urology was consulted for possible stent or nephrostomy placement to prevent further renal injury. Intervention was ultimately deferred given improvement of creatinine over the hospitalization with medical management. The patient also had a profound anion gap metabolic acidosis which improved with the patient’s acute kidney injury. Patient was discharged on RIPE therapy with oversight from the local public health department.However, the patient again presented to the ER less than a month later for worsening acute kidney injury with initial creatinine of 5.40 mg/dL. He was diagnosed with type 1 renal tubular acidosis (RTA) and recurrent hypercalcemia secondary to renal tuberculosis. He was treated aggressively with bicarbonate and potassium containing fluids and was recommended by Nephrology to have a percutaneous nephrostomy tube to prevent further renal compromise. Urology was consulted, and a MAG-3 scan was ordered, which showed non-obstructive slow flow, with functionality of 19% of the right kidney and 81% of the left kidney. Ultimately, intervention was again deferred given significant improvement in kidney function with medical management. The patient was discharged with scheduled outpatient appointments to nephrology and urology.
Discussion: This case illustrates the potential for severe multiorgan involvement of disseminated tuberculosis and the value of a complete inpatient diagnostic work-up and multidisciplinary collaboration in the hospital setting. Although multiorgan involvement (particularly renal involvement inciting renal tubular acidosis) as seen in this patient is rare, recognition of this syndrome is critical to application of appropriate therapy and education for future inpatient clinicians in guiding management, particularly for patients from endemic areas like Latin America or Asia (3).
Conclusions: Miliary tuberculosis provides a unique diagnostic challenge to clinicians given the diversity of clinical presentations with potential pulmonary and extrapulmonary organ involvement (1). Although a rare condition in general, the condition is more frequent in endemic areas and individuals with certain risk factors, such as those with diabetes, ESRD, history of immunosuppressive drugs, or other immunocompromised states (2). Through coordinating care in the inpatient setting while ordering the appropriate diagnostic modalities, hospitalists may dramatically improve the morbidity of inpatient cases of acute, disseminated tuberculosis.