Background: Adverse drug events (ADEs) are common and dangerous in the hospital. One cause of ADEs is medication regimen inappropriateness, including polypharmacy, drug-drug interactions, and medications that are inappropriate or inappropriately dosed given patient’s age, renal, and hepatic function. Inpatient pharmacists are medication experts and often round with medical teams, but they may not have information readily available to make optimal recommendations regarding medication appropriateness. Our goal was to implement and evaluate real-time clinical decision support (CDS) regarding medication regimen appropriateness among inpatient pharmacists.
Methods: We conducted a prospective pre-post time-motion study at two large academic medical centers. We consented and enrolled 10 inpatient pharmacists who round with general medicine service teams. Enrolled pharmacists were provided training and access to Synapse Medicine’s CDS, which could pull medication and clinical information from each hospitals’ electronic health record (EHR) but was accessed as a stand-alone application. Synapse provides appropriateness recommendations based on validated criteria and/or best evidence. Pharmacists were instructed to use the software as they saw fit during inpatient rounds, including conveying Synapse recommendations to the medical team. Trained research assistants utilized TimeCaT time-motion software to track activities of the pharmacists during inpatient rounds on 40 weekday shifts per site for 6 months pre-implementation and 6 months post-implementation. They tracked number, type, and reason of medication recommendations, and time spent using drug references, including Synapse Medicine. The primary outcome was number of recommendations per patient. Secondary outcomes were time spent using reference software per patient and per recommendation. We compared outcomes pre- vs. post-implementation using descriptive statistics followed by generalized linear mixed models, using Poisson regression (primary outcome) and linear regression (secondary outcomes) and random effects by pharmacist. We also descriptively analyzed types of recommendations made.
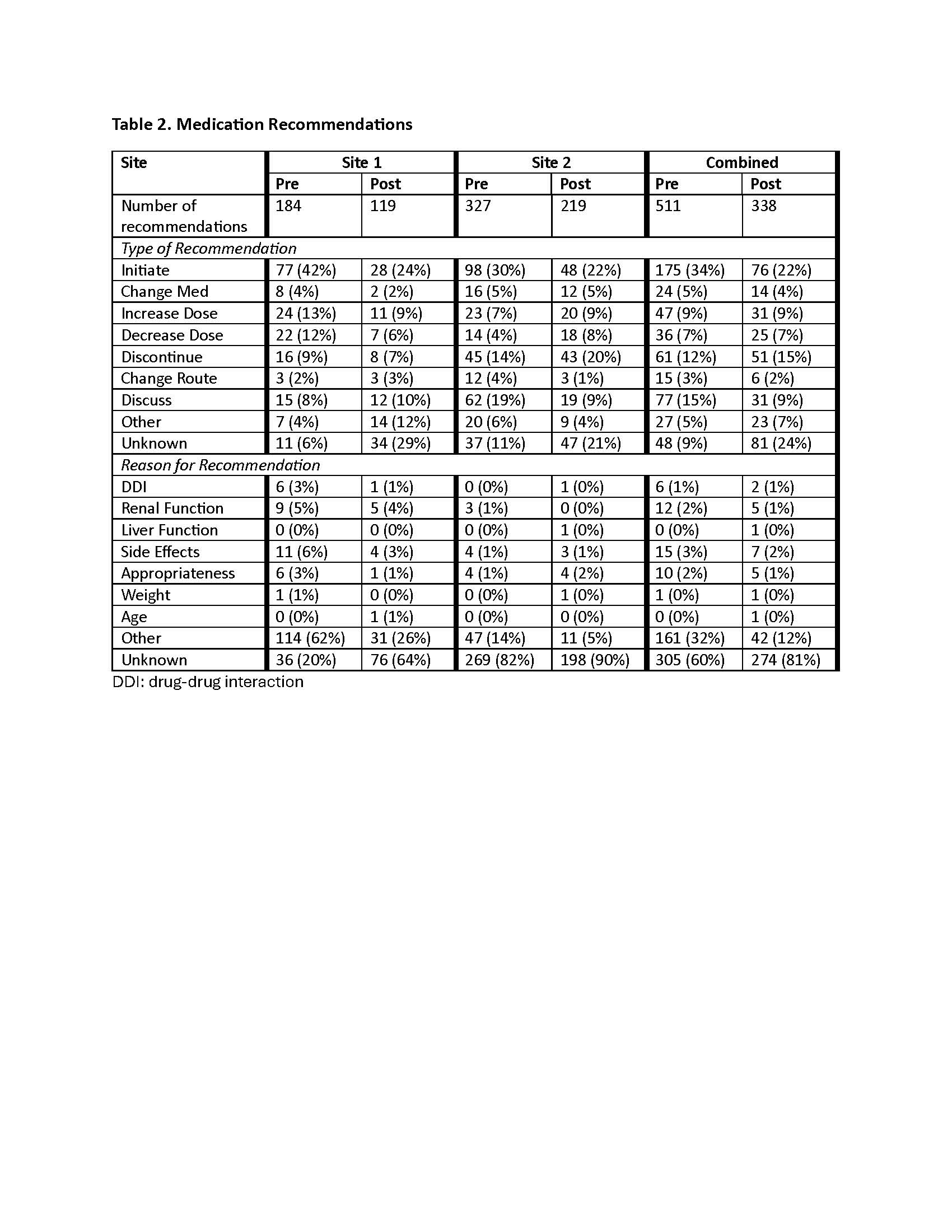
Results: Use of Synapse was more common at site 2 (267 uses on 181 patients) than at site 1 (42 uses on 33 patients). At site 1, there were small (and statistically insignificant) decreases in the number of recommendations and increases in time spent using reference software (per recommendation and per patient) during the post-implementation period. At site 2, these differences were more pronounced, with significant increases in time spent (Table 1).Across both sites, there were 511 recommendations pre-implementation and 338 post-implementation. The proportion of recommendations to initiate medications decreased from 34% to 22%. The proportion of medication discontinuations increased from 12% to 15% (Table 2).
Conclusions: Use of a commercially available CDS by inpatient pharmacists was associated with a small decrease in medication initiations and slight increase in medication discontinuations, consistent with the conservative, safety-focused approach of the CDS. Use was also associated with an increase in time spent per recommendation, especially in the site that used it more, possibly leading to decreased number of recommendations. Future evaluation is needed to determine whether full integration of the CDS into the EHR improves clinical efficiency.
.jpg)