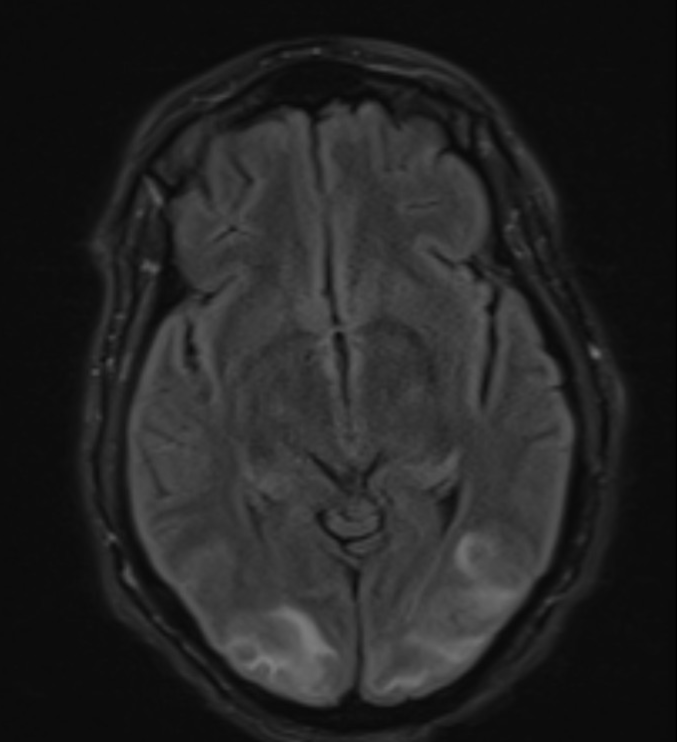
Case Presentation: A 52-year-old woman presented to the emergency department with altered mental status, headaches, and bilateral visual loss. She was admitted a month prior due to severe anemia with hemoglobin of 1.6 grams per deciliter resulting from chronic menorrhagia. She had received multiple blood transfusions at that time.On presentation, her blood pressure was 130/62 mm Hg. The patient was oriented only to person and place. She was found to have left gaze deviation and bilateral vision loss with no focal neurological deficit. A computed tomography scan of the head without contrast was negative for hemorrhage or ischemic changes. The patient was admitted to the neurocritical care department for status epilepticus and was started on antiepileptics. Magnetic resonance imaging (MRI) of the brain showed interval development of posterior reversible encephalopathy syndrome with small acute ischemic infarcts in the left frontal and bilateral parietal lobes. The patient was treated supportively with antiepileptics, which improved her condition. At the time of discharge, she had some residual dysarthria, right dysmetria, and left sixth cranial nerve weakness.
Discussion: The etiology of posterior reversible encephalopathy syndrome (PRES) is diverse, involving factors such as severe hypertension, eclampsia/preeclampsia, cytotoxic and immunosuppressive medications, renal failure, autoimmune conditions, and toxins (1). Common symptoms include headaches, altered mental status, seizures, and visual disturbances. Blood transfusion leading to PRES is rare and has been sparsely described in the literature (2,3). It is assumed that there is a baseline cerebral vasodilation in patients with chronic anemia. Blood transfusions increase blood flow and viscosity, resulting in reflex generalized cerebral vasoconstriction leading to PRES (2). In the setting of relevant clinical symptoms, an MRI of the brain is the imaging modality of choice to diagnose PRES (1). Treatment of PRES includes seizure monitoring, prevention with antiepileptic agents, discontinuation of the causative agent if possible, and prevention of electrolyte abnormalities and hypo or hyperthermia (4). In recent studies, PRES shows a mortality rate of around 19% and persistent neurological deficit in 44% of cases (1).
Conclusions: Given the infrequent occurrence of PRES after blood transfusion, clinicians should exercise vigilance for neurological complications in patients with chronic anemia undergoing transfusions.