Background: Within the medicine service line (MSL) at Memorial Hermann Hospital TMC, the average length of stay (LOS) is 6.53 days. Despite this duration, discharge education is frequently deferred until the day preceding discharge or the day of discharge. Furthermore, there is no standardized protocol to evaluate patient readiness to receive educational content, ensure the presence of family members or designated caregivers during the session, or systematically assess comprehension of the information provided.
Purpose: This project aims to implement a Complex Care Discharge Coordinator (CCDC) role within the Medicine Service Line (MSL) to enhance discharge education and care coordination for high-risk patients transitioning home or home with home health services. The CCDC will utilize evidence-based strategies to deliver timely, structured, and patient-centered education, ensuring readiness to receive information, caregiver involvement, and comprehension of discharge instructions. By integrating this dedicated role, the initiative seeks to improve care transitions, reduce post-discharge complications, and reduce preventable readmissions.
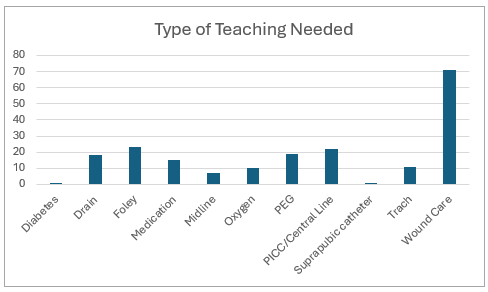
Description: The Complex Care Discharge Coordinator (CCDC) supports six units within the Medicine Service Line (MSL) and focuses on high-risk patients discharging home or home with home health services. Eligible patients include those with complex needs such as wounds, drains, PEG tubes, PICCs, or tracheostomies. The CCDC conducts a comprehensive assessment of each patient’s cognitive function, learning ability, and preferred learning style, while also identifying the primary caregiver responsible for post-discharge care. Educational sessions are scheduled accordingly, and a pre- and post-education survey is administered to evaluate the effectiveness of teaching. Documentation of completed education is entered into the electronic health record (EHR). Based on post-survey results, additional visits are arranged as needed, incorporating supplementary educational materials and alternative teaching modalities to reinforce understanding and promote safe transitions.During the pilot, a total of 283 patient encounters were documented, encompassing teaching, scheduling, and coordination activities. After removing duplicate entries, 193 unique encounters were identified, representing 183 individual patients, five of whom experienced two separate hospitalizations. Across these encounters, 198 teaching sessions were completed. Among the 193 unique patients, 47 experienced readmission within 30 days, corresponding to a 24.3% readmission rate. Patient experience feedback was limited, with only 12 of the 183 unique patients returning surveys. Of these respondents, 7 were promoters, 3 were passive, and 2 were detractors, suggesting generally positive engagement with the discharge education process.
Conclusions: Discharge education should be implemented as a comprehensive, systematic process rather than a last-minute intervention. Effective education must incorporate patient-specific factors, including readiness to receive information, preferred language, and cognitive or health literacy considerations. These factors should guide the methodology, the materials provided, and the timing of delivery, while ensuring the presence of caregivers or medical power of attorney (MPOA) when appropriate. Standardizing these elements is essential to improve patient understanding and enhance transitions of care.