Background: Medication reconciliation errors remain a major driver of preventable harm, particularly during hospital admission when incomplete medication histories lead to missed therapy, duplicate treatment, or incorrect dosing. National data show that medication discrepancies occur in up to seventy percent of patients and contribute to adverse drug events and readmissions. At our institution, baseline audits revealed very low accuracy when medication histories were collected by clinicians or nursing staff, highlighting a need for a more structured approach to this patient safety process.
Purpose: To evaluate the impact of introducing trained pharmacy technicians to perform admission medication history intake on accuracy rates and discrepancy reduction.
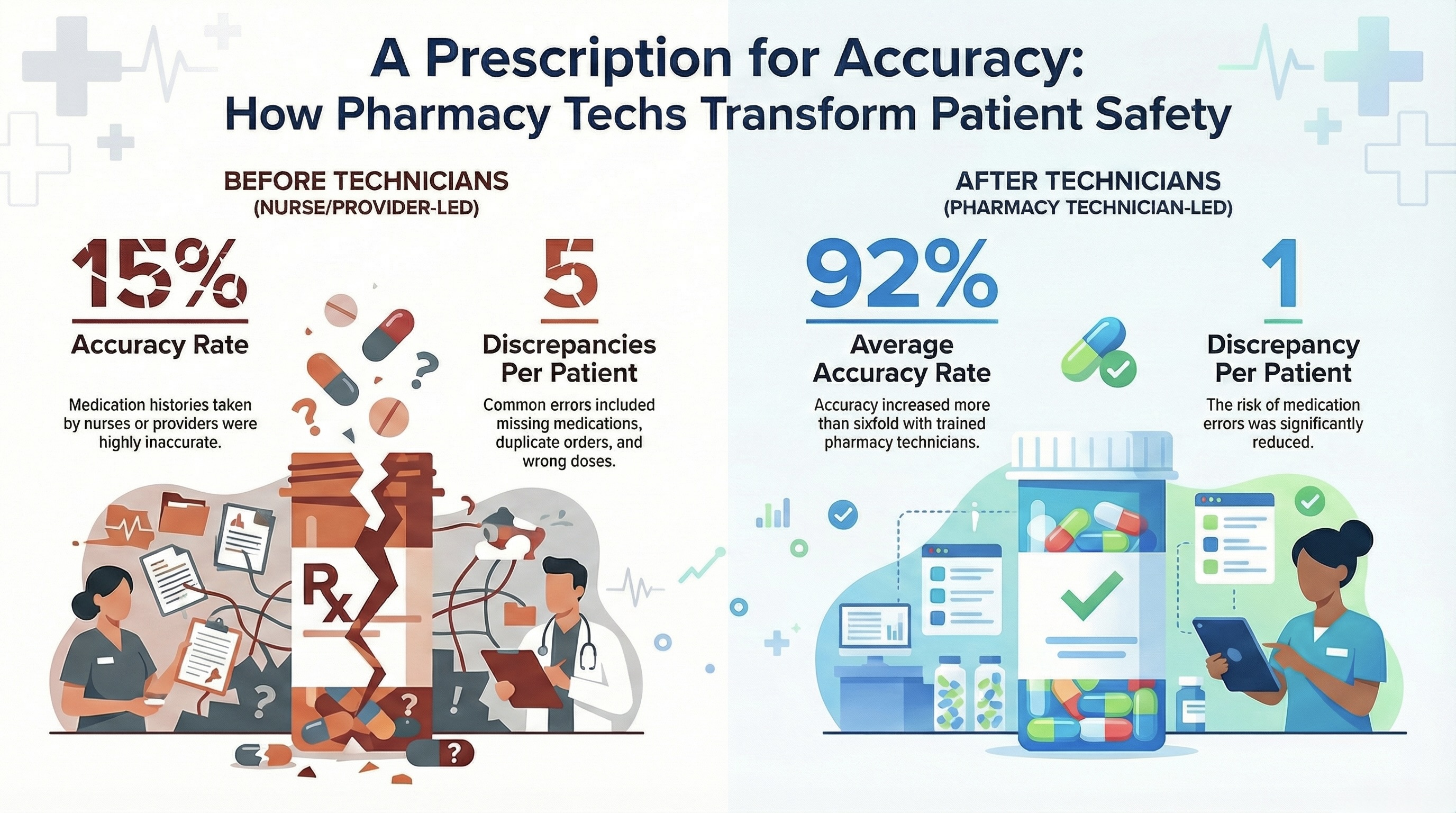
Description: This quality improvement project assessed medication history accuracy from September two thousand nineteen through September two thousand twenty four at a single tertiary care center. Prior to the intervention, medication histories were completed by nurses or clinicians and demonstrated accuracy rates near fifteen percent. In March two thousand twenty one, a pharmacy technician medication history program was introduced and progressively expanded from three to seven technicians, ultimately covering patients fifty five years and older. Technicians received structured training and collected medication histories daily from zero seven hundred to twenty three hundred hours. Transitions of care pharmacists audited ten percent of cases monthly to verify accuracy. Discrepancies were categorized as missing medications, duplicate or no longer taking medications, and incorrect dose or directions. The post technician accuracy metrics were compared to the pre technician period.
Conclusions: Implementing a dedicated pharmacy technician medication history service markedly improved the accuracy of admission medication reconciliation. Accuracy increased from fifteen percent pre intervention to more than ninety percent post intervention, and discrepancies decreased from an average of five per patient to one. This model demonstrates that trained pharmacy technicians significantly enhance medication safety and reduce errors during transitions of care. Future work may include expanding technician roles to discharge reconciliation, integrating outpatient pharmacy records, and evaluating outcomes across multiple institutions to strengthen generalizability.