Case Presentation: A 76-year-old Caucasian male with a past medical history of essential hypertension and type II diabetes mellitus presented with groin pain, nausea, vomiting, and right lower quadrant (RLQ) abdominal pain. The patient’s labs showed a high neutrophil count (82.3) and leukocytopenia (7). CT scan of the abdomen showed an abnormality of the mid sigmoid colon and small bowel extending to the ileocecal valve and base of cecum. A potential diagnosis of appendicitis was suggested with possible development of multifocal abscesses and potential small bowel to colonic fistula.The patient subsequently underwent a diagnostic laparoscopy, however the appendix could not be visualized. After transition to an open procedure, the appendix was identified and was described as being enlarged and gangrenous at the site of perforation. It was determined to be the source of the abscess cavity. It was suctioned out and irrigated. The pathology report showed goblet cell shaped epithelial cells consistent with Goblet cell Carcinoid and the patient underwent a right hemicolectomy The GCC was found to be stage IIb. It was recommended that the patient to follow up with outpatient oncology team to undergo a CT scan for hepatic evaluation and a colonoscopy due to 42% of patients with this neoplasm having a concurrent colorectal neoplasm.
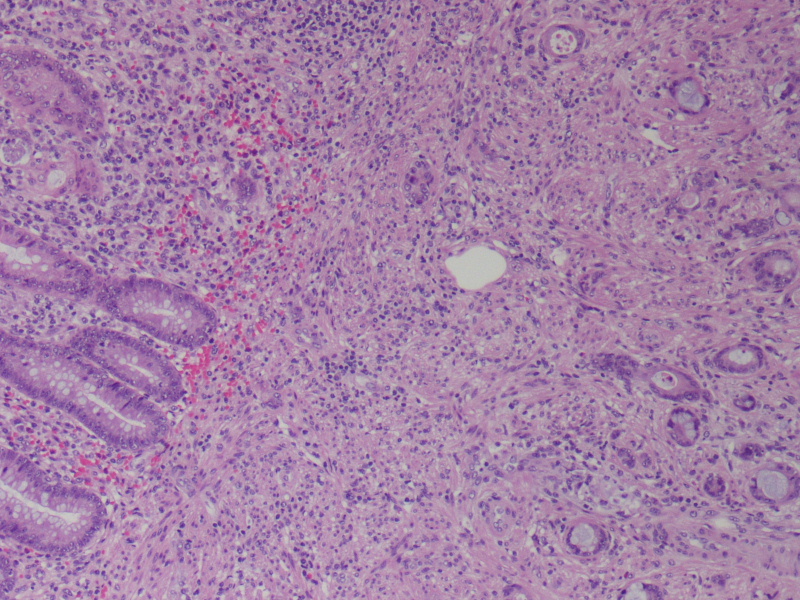
Discussion: Goblet Cell Carcinoid (GCC) of the Appendix is a rare tumor which affects 0.01 to 0.05 per 100,000 people per year. While patients are typically in the fifth decade of life presenting with appendicitis (32%) or abdominal pain (20%), up to one-third of cases are incidentally found during an appendectomy. A PubMed study [PMID:26356507] indicated that 80% of patients with abdominal pain had a perforated tumor and 88% of these tumors were stage I or II. GCC is identified through histological staining with periodic acid-schiff (PAS) stain which shows mucin-containing goblet cell shaped epithelial cells, located in the lamina propria, or submucosa of the appendix while the mucosa stays largely intact.Some current treatment recommendations include a complete right hemicolectomy within three months of the appendectomy, while others suggest not doing one at all. As of now the Neuroendocrine Tumor Society recommends this procedure for the treatment of GCC of any stage.
Conclusions: Our treatment of this patient demonstrates the viability of a right hemicolectomy in the treatment of GCC of the Appendix. The patient’s staging also confirmed that for most patients, at time of diagnosis, specimens are at Stage I or II as our patient was Stage II. However, the role of chemotherapy, and post-operative follow up protocols need further study.