Background: Bedside nurses often communicate via alphanumeric (text) paging with hospitalists and other providers. To help the nurse and provider triage the urgency of these messages, our institution has implemented a tiered paging labeling system based on message priority, but the use of this labeling system and the concordance between provider perception and nurse perception regarding message priority is unknown. In this study, we investigated the number of text pages sent from nurses to hospitalists that included labeling to indicate message priority and assessed the concordance between nurse priority classification and hospitalist priority classification in labeling these messages.
Methods: We analyzed text pages sent through an electronic paging system from nurses to hospitalists working on the direct care medicine service at a large, urban academic medical center over a 5-week period. Labels indicating message priority included “FYI” (i.e., for your information, no action required), “ACTION” (i.e., action required, non-urgently), and “911” (i.e., urgent action required). Two hospitalists reviewed a randomized subset of these messages masked to the original priority label and independently assigned labels of “FYI”, “ACTION”, or “911” to these messages. A third, senior hospitalist served as a tiebreaker in the event of disagreement between the two reviewers. Hospitalist ratings were then compared to the original label indicating message priority as characterized by nursing.
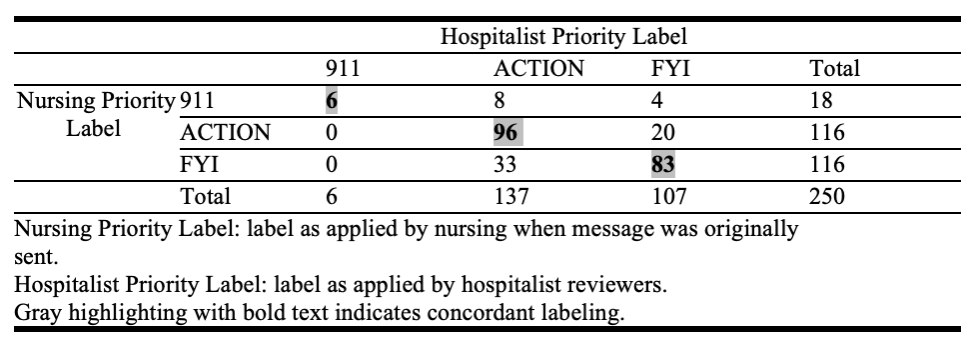
Results: From October 1, 2023 to November 9, 2023, the average daily census on the direct-care hospital medicine service was 75.3 patients for 9 hospitalist teams. Over this time period, nurses sent 7,211 pages to hospitalists through the electronic paging system. Of these, 18 (0.25%) were labeled “911” pages; 3,831 (53%) were labeled “ACTION” and 2,710 (38%) were labeled “FYI.” The remainder of the messages (652, 9%) did not include a label indicating priority. 250 messages masked to their original priority labels were reviewed. The two hospitalist reviewers were outstanding in their agreement about priority classification assignments (kappa 0.80, p< 0.0001). The senior hospitalist reviewer adjudicated 26 (out of 250) discrepancies. The final hospitalist priority classification and the nursing priority classification exhibited moderate agreement (kappa 0.52, p< 0.0001); hospitalists were more likely to label messages as “ACTION” than either “911” or “FYI” (Table 1). A small number of pages (n=4) labeled by nursing as “911” were labeled by hospitalists as “FYI.”
Conclusions: In our single institution study, we found that nurses who text-paged hospitalists rarely used the most urgent priority classification label in their messages, and a considerable proportion of messages were informational in nature. Hospitalist reviewers exhibited moderate agreement with the original priority labeling applied by nurses, with a tendency to consider more messages actionable than either urgent or informational. Possible explanations for this discordance include variable interpretations of urgency and patient-specific clinical contexts being unknown to the masked reviewers. Our results highlight that there are opportunities to improve alignment of paging priority labeling between disciplines to improve physician nurse communication.