Background: The Warren Clinic Hospitalist Department oversees adult inpatient admissions for the Saint Francis Health System in Oklahoma, comprising over 140 clinical FTE’s. The department handles approximately 40,000 discharges annually across several acute facilities. The health system has seen unprecedented challenges recently due to COVID-19, staffing shortages, and an increasingly older population. These challenges increased Length of Stay for hospitalist patients 15.29% from fiscal Year 2020 to 2022. This also affected throughput causing delayed discharges, increased ER wait times, and delayed care for patients. Recognizing the impact, the hospitalist department proactively created a multidisciplinary Length of Stay task force. The objectives of the team were to optimize operational workflows, dissect discharge barriers, set best practice standards, streamline throughput, and elevate quality of care.
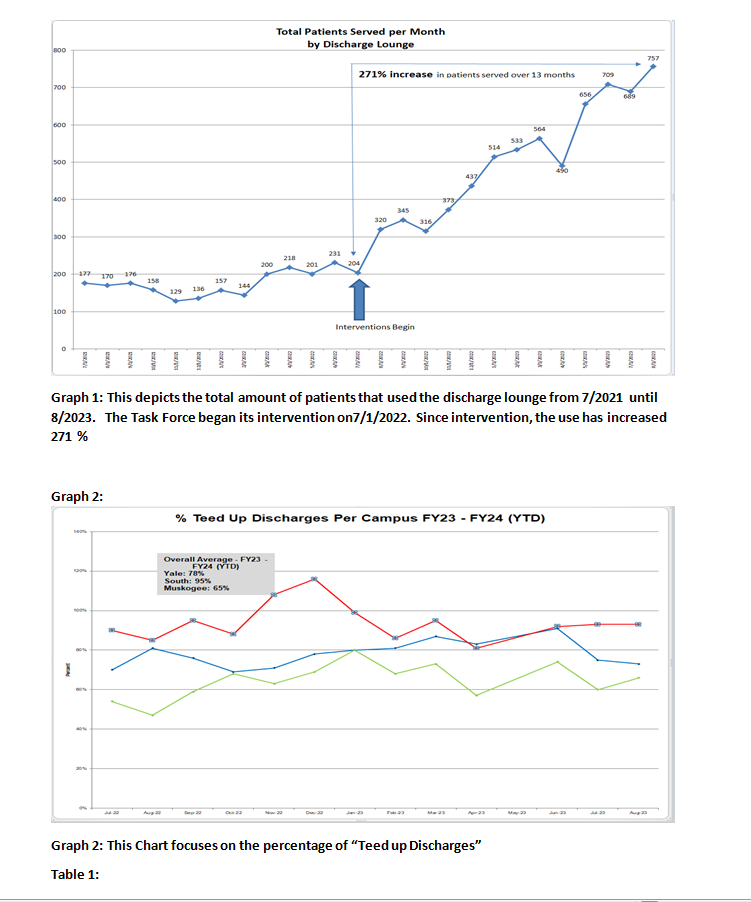
Methods: The task force consisted of key stakeholders from the Hospital Medicine, Case Management and Process Improvement departments. Goals were set to reduce Length of Stay by 0.25 days for the department, enhance throughput by decreasing ER hold hours and increasing the number of transfers accepted by our system, and improve quality outcomes in readmission, complication, and mortality rates. The following process changes were made:1. Monthly tips were sent to providers focused on best practice tips to providers focusing on weekend barriers, early initiation of home health and SNF orders, communication with case management, early documentation of disposition, and early use of mobility protocols. 2. Increase the number of direct admits by revamping the triage process, addressing barriers to direct admission, and engaging PCPs to bypass the ER when referring their patients.3. Elevating the use of our discharge lounge (an area at where patients stay after they are discharged if they are waiting on a family member, etc.) by reformatting criteria and monitoring utilization. (see Graph 1) 4. We set a goal of identifying barriers to discharge early by establishing a 3pm bed huddle between our discharge navigators and case management. We developed and monitored “teed up discharges” as a discharge milestone. (see Graph 2) This milestone promoted identification of potential discharges 24 to 48 hours before discharge allowing early identification of barriers.
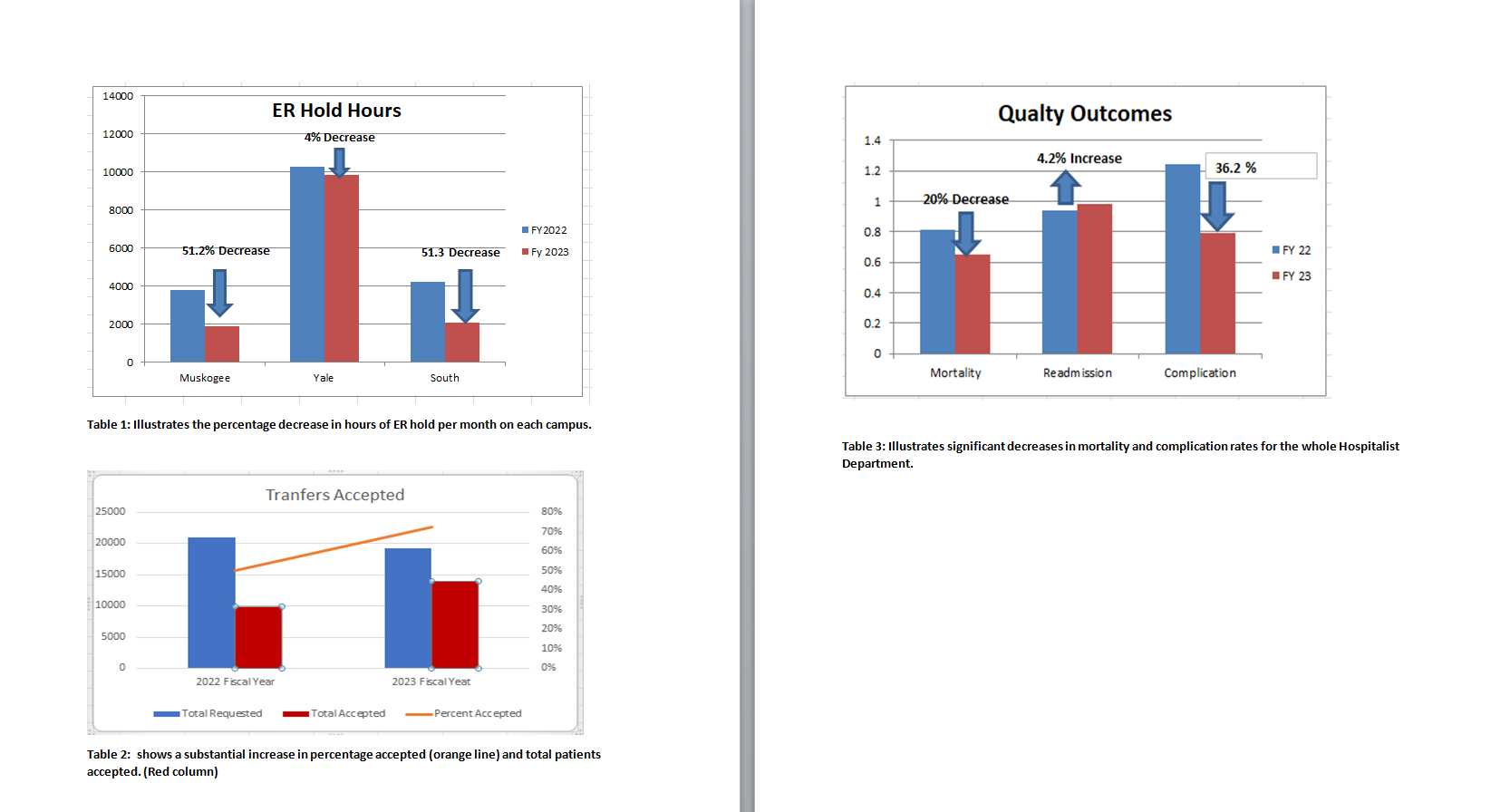
Results: The changes showed significant improvements in all of our throughput measures. This included a decrease in ER hold hours of 4%, 51.2%, and 51.3% at our three acute care campuses. (Table 1.) This occurred in conjunction with each ER having an increase in the total number of visits from Fiscal Year 2022 to 2023. In addition, the percentage and total number of patients accepted increased. (Table 2) Length of Stay in our department decreased 8.4% or 0.51 days throughout our department. (Graph 3) Finally, we had decreases in both our mortality and complication rate by 20 and 36% respectively, with a slight increase in readmission rate (Table 3)
Conclusions: The Hospitalist Length of Stay Task Force was a collaborative initiative started by our Hospitalist Department to address negative trends in Length of Stay, and throughput. The collaborative process changes recommended and implemented by the Task Forced was successful in reducing length of stay and improving throughput while delivering high quality care for all hospitalist patients. The Task Force produced measurable improvements, providing a replicable model for all of hospital medicine.