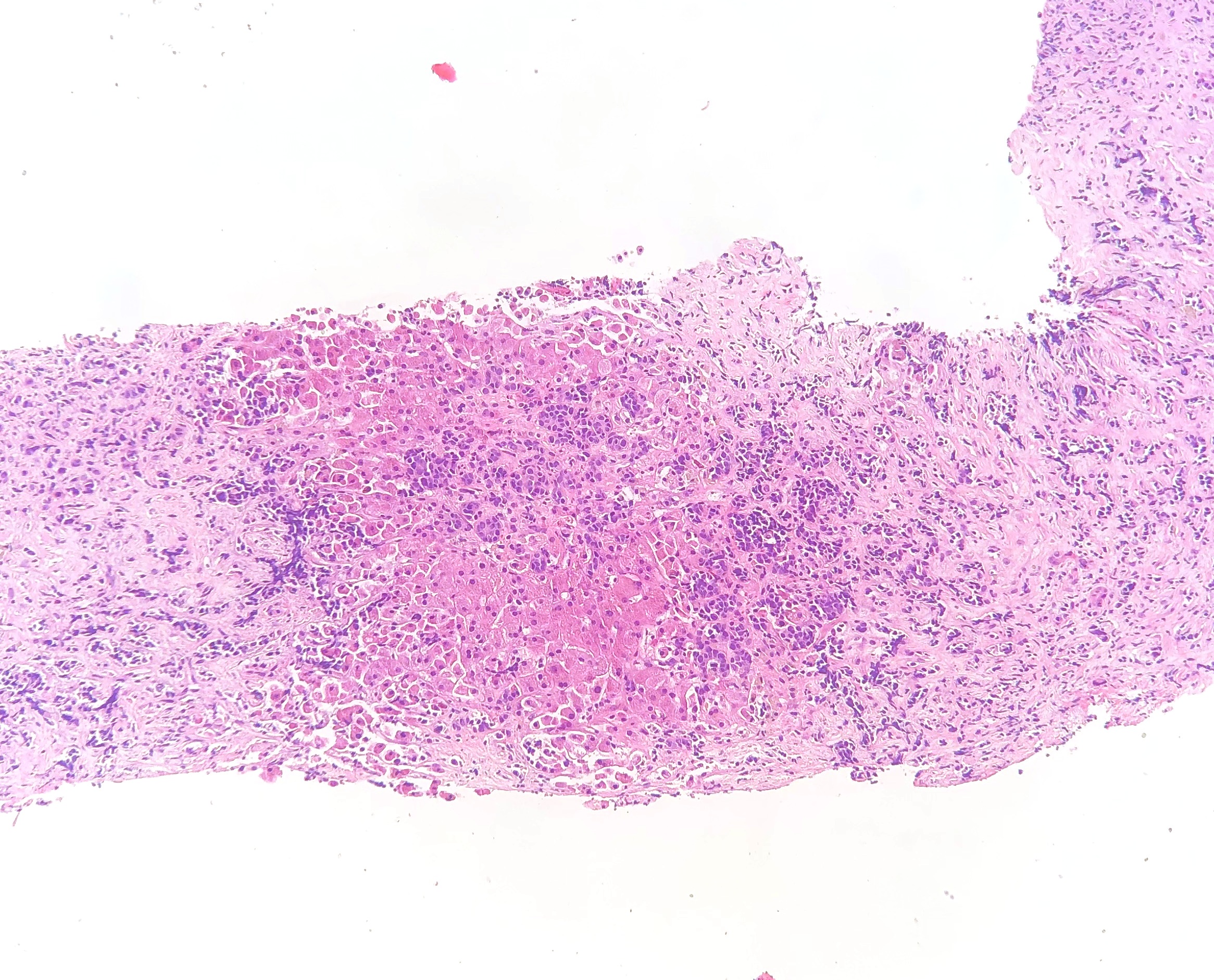
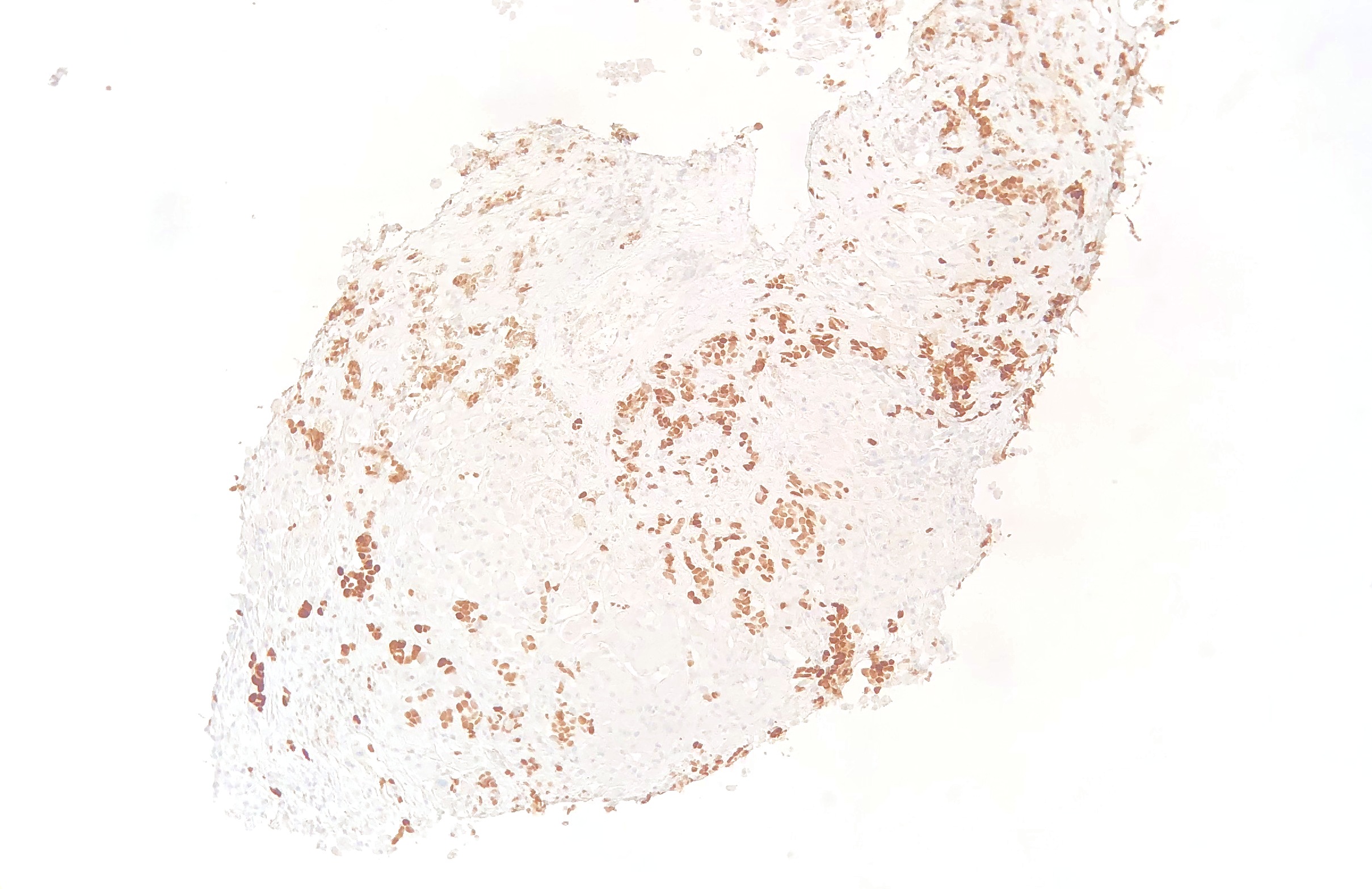
Case Presentation: A 70-year-old female with a history of lobular carcinoma of the breast, status-post mastectomy followed by adjuvant radio-chemotherapy in remission for 4 years admitted with a complaint of right upper quadrant pain and jaundice. Examination was positive for icteric sclera and ascites. Her hemoglobin was 8.8 gm/dL; mean corpuscular volume of 90.5 fL; ferritin of 5485 ng/mL; iron saturation of 74 %; and transferrin of 126 mg/dL; all suggestive of hemochromatosis. Additional labs included aspartate aminotransferase (AST) 240 IU/L; alanine aminotransferase (ALT) 431 IU/L; gamma glutamyl transferase (GGT) 550 IU/L; alkaline phosphatase (ALP) 431 IU/L; total bilirubin (TBili) 11.6 mg/dL; direct bilirubin (DBili) 6.7 mg/dL; and INR 1.8. Computed tomography (CT) scan of the abdomen showed ascites and heterogeneous attenuation of the liver suggestive of cirrhosis. An extensive workup including magnetic resonance (MR) abdomen, viral serologies (HAV, HBV, HCV and CMV), paracentesis, and autoimmune and metabolic studies failed to identify an etiology. After four days in the hospital, she developed clinical hepatic encephalopathy with ammonia of 94 μmol/L and associated bleeding diathesis from intravenous catheter sites. Her TBili increased to 16 mg/dL with DBili of 9 mg/dL. A working diagnosis of hemochromatosis was pursued. A trans jugular liver biopsy revealed poorly differentiated carcinoma consistent with metastasis from breast primary (Figure 1,2). The patient’s condition deteriorated, hepatic encephalopathy progressed, and the patient died within a week following the onset of acute hepatic failure. DNA testing revealed patient was heterozygous for H63D mutation.
Discussion: Most individuals with hereditary hemochromatosis are homozygous for the C282Y or H63D mutation. However, our patient’s genetic architecture consisted of one copy of H63D (heterozygous), which has no associated risk for hemochromatosis.[1] Nevertheless, studies have shown that presence of a heterozygous H63D mutation results in a significant increase in serum transferrin saturation and alters iron indexes without significant iron overload.[2, 3] The most common pattern of liver metastasis is the formation of discrete multiple nodules. A single nodule formation is next most common, while diffuse tumor invasion into the liver parenchyma is less common.[4] The clinical presentation, the blood testing pattern of a hemochromatosis phenotype and radiological evidence in our patient obscured the malignant infiltration of the liver until tissue biopsy was obtained. Early recognition and diagnosis at presentation will help avoid battery of investigations and help providers convey vital information, such as prognosis and scarcity of treatment, to their effected patients.
Conclusions: Diffuse parenchymal metastasis is an unusual pattern of liver metastasis that can cause liver failure.[5] CT scan and MR of the abdomen failed to detect liver metastasis; while microscopic examination revealed diffuse tumor cells. In cases of acute liver failure with suspicion of malignancy, liver biopsy should be obtained to evaluate an infiltrative hepatic disease.