Background: Clostridium difficile associated diarrhea (CDAD) is an infectious diarrheal illness associated with high morbidity and mortality. Patients with CDAD have diarrhea symptoms and a positive test for a toxin-producing Clostridium difficile organism. However, patients may be asymptomatic carriers without diarrhea or symptoms of clinical Clostridium difficile infection and have a positive test. Approximately 10 percent of hospitalized patients are asymptomatic carriers who, if tested, would test positive. Thus, testing of asymptomatic patients is likely to produce some positive results, subjecting patients to unnecessary treatment, and falsely inflating the count of hospital-acquired CDAD. We hypothesized that reducing inappropriate tests on asymptomatic patients, who might be asymptomatic carriers, may reduce the rate of hospital-acquired CDAD.
Methods: At a large, urban, academic health system we used Quality Improvement Methodology including Plan-Do-Study-Act (PDSA) cycles to reduce unnecessary testing. A self-stewardship system for testing was implemented with daily unit-based review of orders and improved interdisciplinary communication about symptoms, primarily diarrhea. We used run charts to follow the average number of Clostridium difficile tests performed weekly as well as the rate of hospital acquired Clostridium difficile per 10,000 patient days as defined by the Center for Medicare and Medicaid Services (CMS). Standard Quality Improvement interpretation of run charts was performed. In addition, comparisons between the pre intervention and post intervention periods were tested using Wilcoxon Rank Sum Tests.
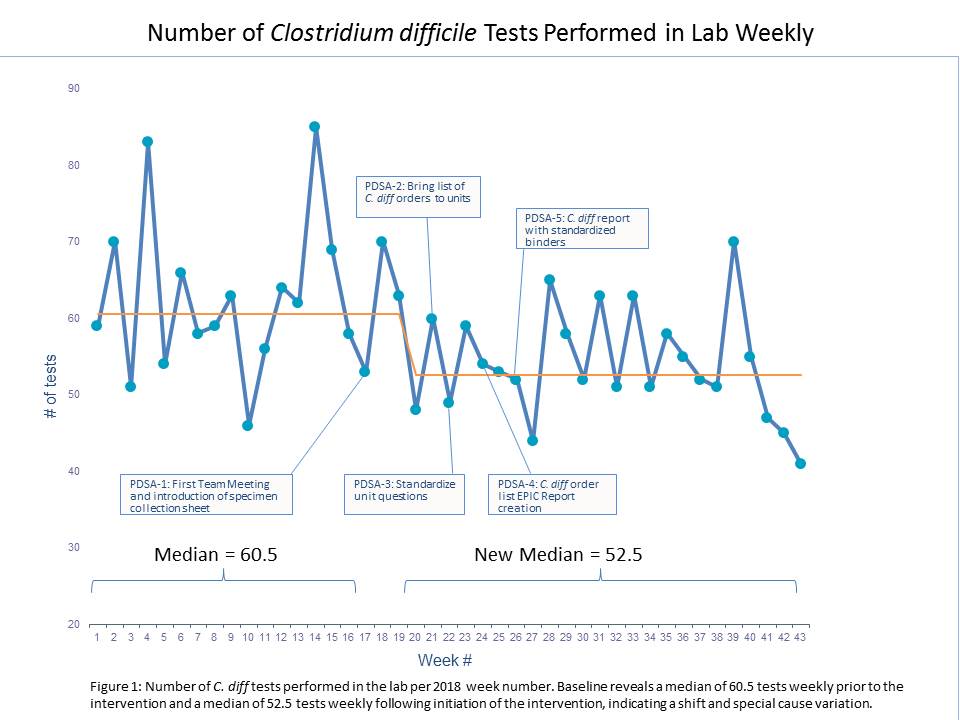
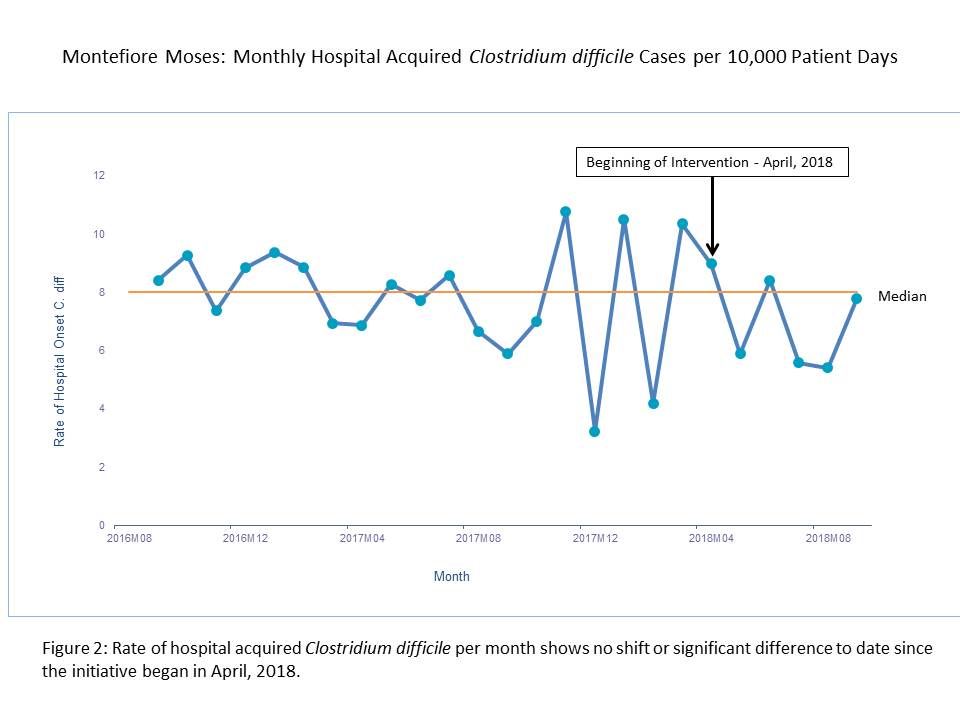
Results: There was a sustained reduction in the number of Clostridium difficile tests performed in the laboratory from a baseline median of 60.5 to 52.5 weekly (Figure 1, p=0.003), indicating a shift consistent with special cause variation. If generalized annually, this improvement would result in over 400 fewer Clostridium difficile tests performed yearly. The monthly rate of hospital onset Clostridium difficile cases per 10,000 patient days as defined by CMS did not reveal a shift in the median nor was there a statistically significant difference between the pre and post intervention periods (Figure 2, p=0.14).
Conclusions: A Self-stewardship program focused on reducing unnecessary Clostridium difficile testing resulted in a significant reduction in Clostridium difficile testing performed in the lab. However, the reduction in testing has not translated into a significant reduction in the rate of hospital acquired Clostridium difficile cases.