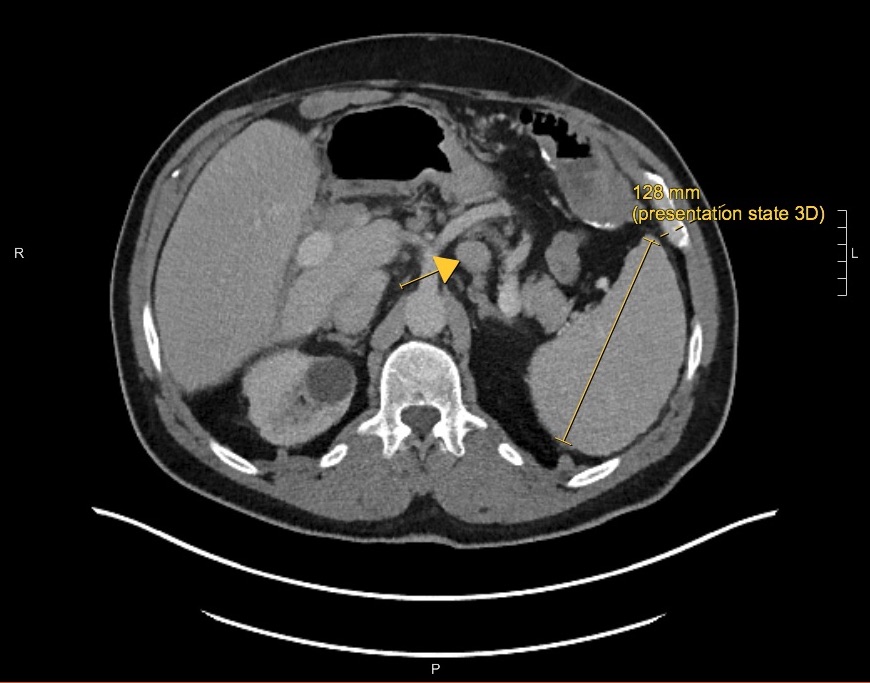
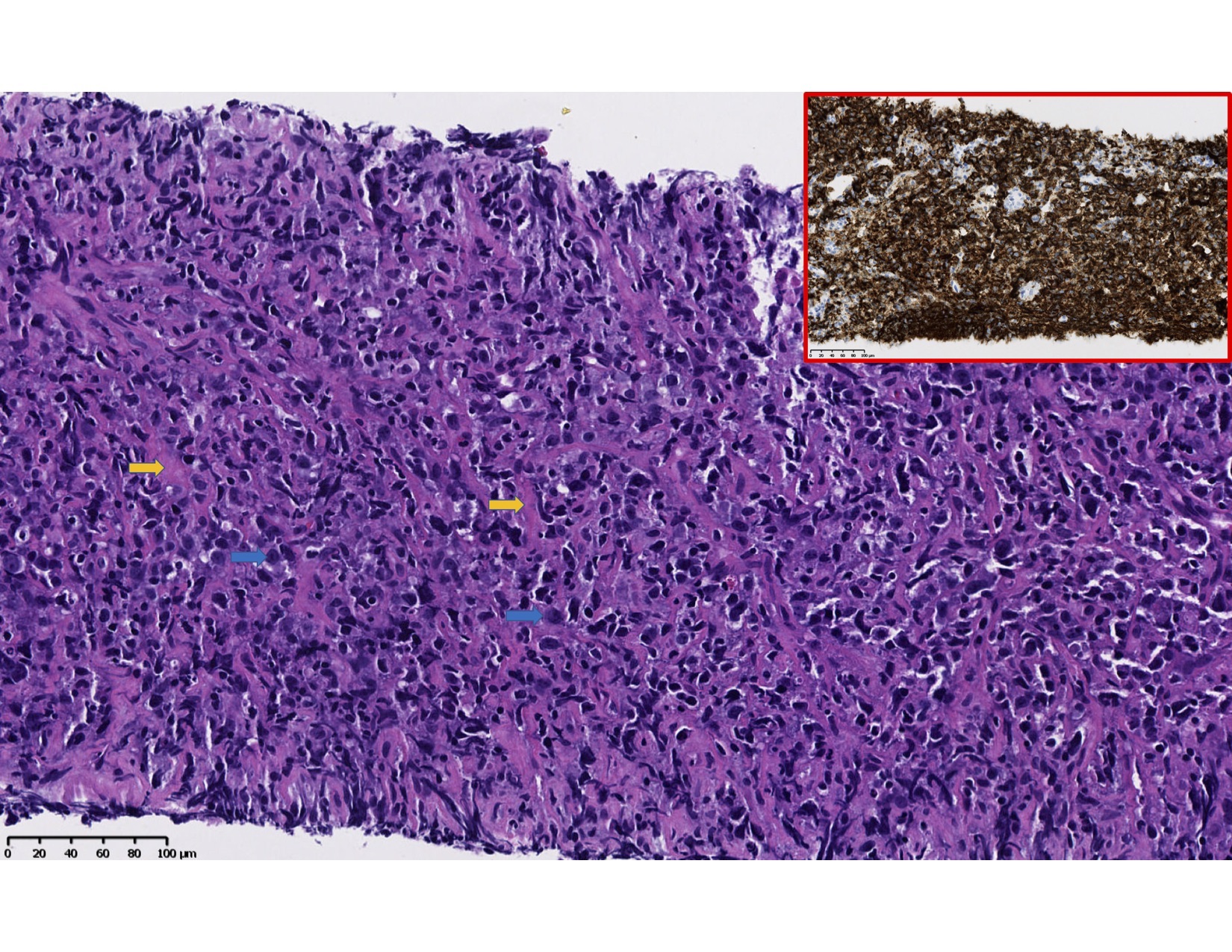
Case Presentation: A 60-year-old male presented with one week of new onset fevers and fatigue. Past medical history included primary sclerosing cholangitis, orthotopic liver transplant 12 years ago and Epstein-Barr virus (EBV) negative post transplant lymphoproliferative disease (PTLD) with partial response to single-agent Rituximab treatment one-year prior.The patient reported debilitating fatigue, daily low-grade fevers, night sweats, non-productive cough, headache, anorexia and epigastric pain for one week. He had no outdoor exposure, travel or sick contacts. Physical exam elicited palpable splenomegaly however no lymphadenopathy, jaundice or rash. Labs were notable for acute pancytopenia and CT scan showed splenomegaly with hypoattenuating lesions as well as intrabdominal lymphadenopathy (Image 1). The patient was treated with fluid resuscitation and empiric antibiotics. He had a negative infectious work up including EBV testing. Flow cytometry was significant for 9% lymphocytes including polyclonal B-Cells. A core biopsy of a mediastinal lymph node had effacement of normal lymph node architecture by sheets of large atypical lymphocytes and sclerosis (Image 2). Immunohistochemical analysis confirmed the B-cell lineage of these cells (+CD20) with a high proliferation index (+Ki67) and negative EBV. The patient was diagnosed with EBV negative diffuse large B-cell lymphoma (DLBCL), an aggressive disease requiring prompt initiation of chemotherapy.
Discussion: This case presentation was initially concerning for recurrent PTLD or transformation to high-grade lymphoma verses acute infection in an immunocompromised host. PTLD is the most common malignancy after solid organ transplant, complicating 1.5% of cases.1, 2 PTLD is caused by aberrant lymphoproliferation in the setting of chronic immunosuppression and decreased cancer immune surveillance.1, 2, 3 It includes a wide spectrum of heterogeneous diseases that can progress into high-grade lymphomas.1 PTLD has a biphasic presentation including EBV positive PTLD 0-3 years post transplant and EBV negative PTLD 7-10 years post transplant.3, 4 It is essential that hospitalists consider the diagnosis of PTLD in the differential of transplant patients presenting with B symptoms, lymphadenopathy or signs of graft dysfunction.5 This patient had indolent PTLD with sudden extreme fatigue, worsening lymphadenopathy and pancytopenia, which represented transformation to DLBCL. Hospitalists are essential to the care of solid organ transplant and hematologic malignancy patients with acute decompensations and can ensure a comprehensive evaluation including infectious disease testing, PET scan, flow cytometry and excisional lymph biopsy.5 Hospitalists may also be able to help prevent PTLD, as regular evaluation and treatment for EBV may be protective in post transplant patients.3, 5
Conclusions: This case emphasized important learning objectives in hospital medicine such as: to include hematologic malignancy early in the differential diagnosis and work up in post-transplant patients; identify immunosuppression as a risk factor for hematologic malignancy; recognize the biphasic presentation of PTLD and association with EBV; and to learn possible preventative measures for PTLD.