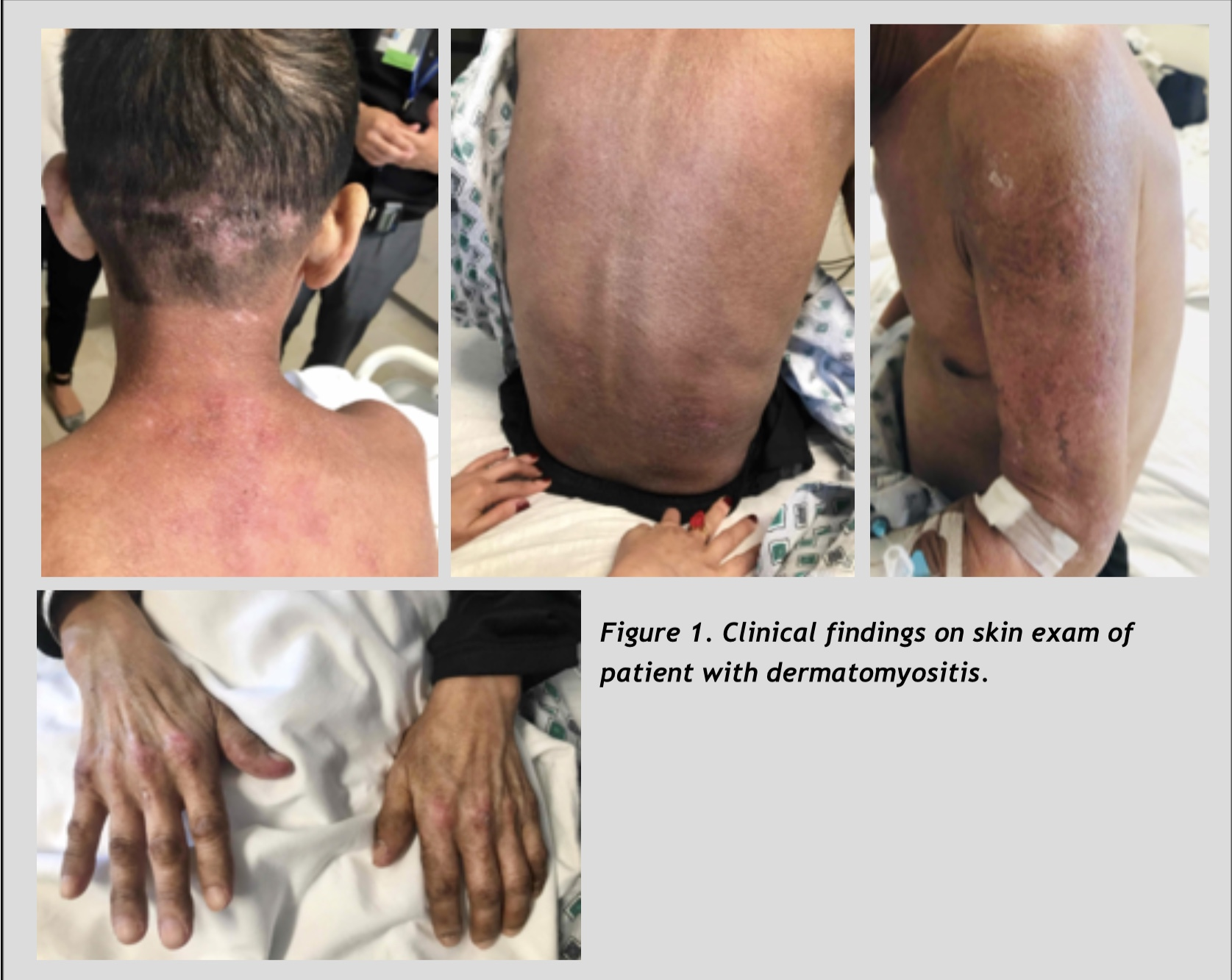
Case Presentation: 49-year-old man with history of alcohol abuse presented with a 3-month history of progressive weakness, weight loss and skin lesions. An outside dermatologist had diagnosed the patient with porphyria cutanea tarda (PTC) one month prior to admission based on characteristic skin findings on physical examination, and elevated urine and serum porphyrin levels. He presented to an outside hospital with failure to thrive, progressive weakness and weight loss despite one month of treatment with Plaquenil. Despite extensive evaluation, no unifying diagnosis was found for the cause of his symptoms. Vitals were stable on transfer. Physical examination was notable for cachexia, erythematous lesions over the MCP joints, and hyperpigmentation of his face, neck, and back. There was proximal weakness of his upper and lower extremities on neurologic exam. His labs were notable for an elevated ESR and CRP, with mildly elevated AST and ALT (with AST > ALT). His CK was normal, comparable to the level tested one month prior. Serum aldolase was elevated. Rheumatology and Dermatology were consulted to evaluate for dermatomyositis. The patient underwent upper extremity skin biopsy, with findings that were consistent with dermatomyositis. MRI of his thighs revealed myositis and muscle biopsy showed tissue necrosis, which confirmed the diagnosis. CT chest/abdomen/pelvis did not show signs of malignancy. Treatment with prednisone was initiated.
Discussion: Dermatomyositis is characterized by proximal muscle weakness with skin manifestations and may be associated with an underlying malignancy. Traditionally, patients have an elevated CK in addition to elevated AST, ALT, and aldolase. In this patient’s case, the normal CK level was assumed to be sufficient to rule out the diagnosis of myositis, delaying appropriate diagnosis and treatment by more than one month. There have been several case studies of patients with dermatomyositis who present with a normal CK, but who have an elevated aldolase levels. Specifically, 25% of patients with dermatomyositis may present with a normal CK. This case report adds further support for the need to test for both aldolase and CK when evaluating a patient with suspected dermatomyositis.
Conclusions: This case illustrates the importance of checking aldolase as well as CK to make the diagnosis of myositis, as CK and other muscle enzymes may not be elevated.