Case Presentation: A 44-year-old woman with past medical history of anxiety, depression, and seizure disorder presented with seizure-like activity consisting of asynchronous bilateral upper and lower extremity shaking, throughout which patient was alert and responsive. Patient had a 5-year history of these episodes, with a recent increase in frequency exacerbated by stress. Prior extensive workup included multiple video electroencephalograms with no epileptiform activity. Patient was prescribed antiepileptics, antidepressants, and anxiolytics to which she was adherent. Patient had no personal or family history of thyroid disease, diabetes, or autoimmune conditions.Later in the hospital course, the patient became obtunded, tachycardic, tachypneic, and hypotensive requiring pressor support and intubation. During episodes, patient had marked anisocoria and increased tone and rigidity in truncal and proximal muscle groups, with flaccid distal muscles and neck muscles, which resolved between episodes. Chest x-ray showed pulmonary vascular congestion and transthoracic echocardiogram showed reduced ejection fraction consistent with stress cardiomyopathy. Labs were remarkable for metabolic acidosis and elevated CK and lactate levels. Initial cerebrospinal fluid analysis was unremarkable. Anti-GAD antibodies were positive (>250 IU/mL) and anti-NMDA antibodies were negative. Patient developed acute DVT requiring anticoagulation, which was then held in the setting of a retroperitoneal hematoma. Patient was treated with plasmapheresis alternating with stress-dose steroids and patient’s neurological and cardiovascular function fully recovered. Patient was discharged in stable condition to an acute rehabilitation facility.
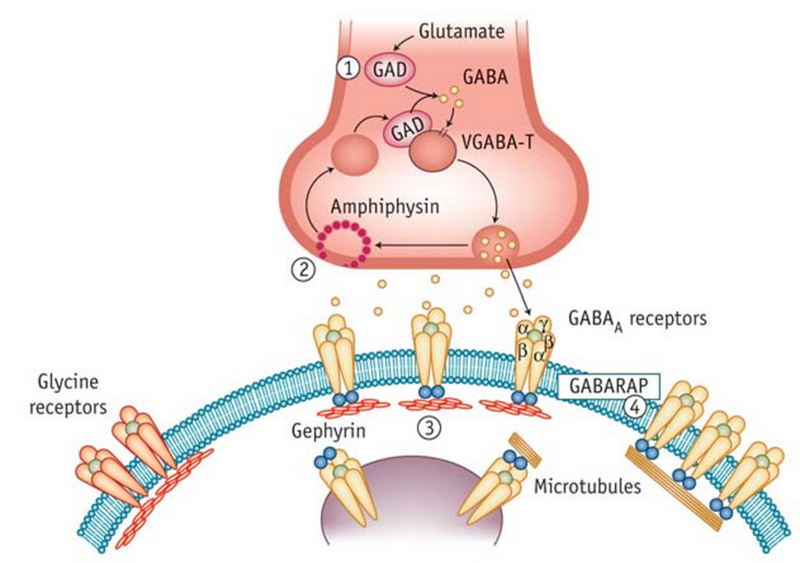
Discussion: Stiff person syndrome (SPS) is a rare (1 in 1 million), progressive acquired neurological disorder thought to be autoimmune in origin. Patients with SPS have very high titers of anti-GAD autoantibodies, which disrupt the neurotransmission and function of GABAergic system, resulting in overstimulation and lack of normal inhibition of antagonistic processes. Electrophysiological studies will show continued co-contractions of both agonist and antagonist muscles resulting in spasms and stiffness. Therapeutic approaches include benzodiazepines for symptomatic relief and immunotherapy.
Conclusions: This patient had previously received significant workup for both epileptic and psychosomatic condition, but there was still significant delay in diagnosis prior to this presentation, resulting in significant distress and exacerbation of her disease. It is important to recognize signs and symptoms, however atypical, to keep this diagnosis on the differential. While IVIG is the preferred treatment for SPS, plasmapheresis in this case was used due to patient’s prothrombotic state. More research on and awareness of this condition is needed to build on our current understanding of the disease and therapeutic options.